Introduction
Auditory temporal resolution or discrimination, in a narrow sense, refers to the shortest duration of time in which the ear can discriminate two different signals.1) As a category of auditory temporal processing, temporal resolution can also be defined by the ability of the auditory system to recognize rapid changes in the envelope of a sound stimulus over time.2) Currently, clinically useful tests to assess temporal resolution are limited, although this is a critical component in accurate auditory perception. Measurement of temporal modulation transfer functions (TMTF) and/or gap detection (GD) threshold has traditionally been used for the identification of temporal discrimination deficits in a variety of clinical populations.3,4,5,6) The Gaps-In-Noise (GIN) test was developed to overcome disadvantages of those previous time-consuming procedures. Recent studies have showed that the GIN test produced solid results in normal-hearing adults,7,8,9) normal children,10) subjects with central auditory disorders,7) and tinnitus patients.11,12) Test performance on a GIN procedure may be the only available psychoacoustic parameter which is truly evaluating temporal resolution and not auditory fusion.
Many researchers have hypothesized that tinnitus "fills in" the silent gap in the background noise when the pitch of the tinnitus is close to the frequency of the noise, and impairments of GD have been considered as a useful tool to objectify the presence of tinnitus in animal models.13) On the basis of this theory, tinnitus is assumed to be present if the silent gap in an ongoing narrow band noise fails to suppress the startle reflex response evoked by an intense noise burst in some animal models. Auditory temporal resolution of patients with severe tinnitus is also expected to be adversely affected by the internal phantom sound in accordance with that paradigm. It is possible that tinnitus interferes with the auditory abilities of temporal resolution, even in individuals with normal hearing levels. A previous study identified the deterioration of auditory temporal resolution by the GIN test in tinnitus patients with normal pure-tone thresholds, compared to normal listeners without tinnitus.11) Subtle peripheral hearing impairment measured in extended high-frequency audiometry and distortion product otoacoustic emission could affect temporal resolution in tinnitus.12)
It is difficult to prove the exact effects of tinnitus itself except for those of hearing disturbance on auditory temporal discrimination of humans, but psychoacoustic abilities of patients with bilateral tinnitus and progressive bilateral sensorineural hearing loss would be quite distinct from those with unilateral tinnitus and ipsi-lesional sudden single sided deafness. Before applying this concept of tinnitus laterality to subjects with hearing loss, we needed to determine whether unilateral tinnitus has influence upon temporal processing. We presumed that unilateral tinnitus hinders the GIN performance in comparison with normal hearing, and therefore the goal of this study was to investigate the effects of unilateral tinnitus on auditory temporal resolution by the GIN test.
Subjects and Methods
Subjects
The subjects were 60 patients (mean age, 43.6┬▒17.6 years; age range, 22-75 years; 27 males, 33 females) (tinnitus group) who had visited our hospital complaining of unilateral tinnitus from 2011 to 2013. All patients were confirmed as having subjective tinnitus in tinnitogram conducted immediately before the GIN test, and showed a symmetric hearing ability Ōēż20 dB HL difference of both ears at whole frequency of 0.25, 0.5, 1, 2, 4, and 8 kHz in pure tone audiometry. Asymmetric hearing was defined as hearing threshold discrepancy greater than 10 dB in more than two consecutive frequencies or greater than 20 dB in more than one frequency in pure-tone audiogram. The controls were 30 people with 60 normal ears (mean age, 42.2┬▒13.9 years; age range, 23-68 years; 11 males, 19 females) (control group) who had never experienced tinnitus and who showed a hearing threshold Ōēż25 dB HL in both ears at every 0.25, 0.5, 1, 2, 4, and 8 kHz. This study was performed with the approval of the Institutional Review Board of our institute.
All patients met the following criteria based on tinnitus case history questionnaires: adults age 18 and older, no history of acute acoustic trauma, no history of ototoxic drug use, no history of otologic disease, and no familial history of hearing loss. Careful examinations of ear, neck, and temporomandibular function were performed to exclude somatic tinnitus or objective tinnitus. Specific tinnitus questionnaires included visual analogue scale (VAS) of tinnitus loudness, where 0 is no tinnitus and 10 is the loudest tinnitus imaginable, and tinnitus handicap inventory (THI). Audiologic tests including pure-tone audiometry, speech audiometry, impedance audiometry, tinnitogram, and the GIN test were investigated. Patients with asymmetric hearing thresholds, Meniere disease, the presence of any tumorous condition, and prior steroid use before study entry were excluded.
Equipments
Gaps-In-Noise (GIN) test
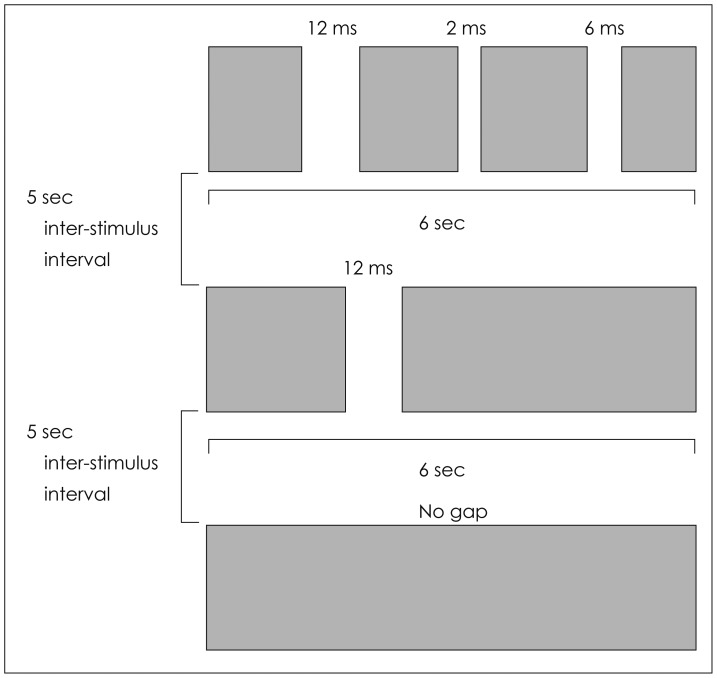
The GIN test was performed to evaluate the temporal resolution as initially proposed by Musiek, et al.7) All subjects were tested while seated in a soundproof room. A compact disk with the recordings of the GIN stimuli was played in a CD player coupled to the audiometer. The stimuli were monaurally presented at 50 dB sensation level (SL) relative to the speech reception threshold. The GIN test is composed of a series of 6-second segments of white noise containing 0 to 3 silent gaps per noise segment. The number of silence gaps in each 6-second of white noise varied from one, two, three or none. The inter-stimulus interval between successive noise segments is 5 seconds and the gap durations presented are 2, 3, 4, 5, 6, 8, 10, 12, 15, and 20 ms (Fig. 1). Four lists were available for the GIN test, and there were 6 noise segments for all time durations of 2-20 ms making total 60 gaps in each list.
The results obtained for each ear were analyzed based on two components of the GIN test, the gap perception threshold and the percentage of correct answers. The shortest gap duration for which there were at least four of six correct identifications (67%) was defined as the GIN threshold. Since there were 60 gaps in each list, the GIN percentage of correct responses was calculated as the percentage of correct responses scored across all gaps: (total number of gaps identified/total number of gaps in the list, i.e., 60)├Ś100 (%).
Pure-tone audiometry
Using a pure-tone audiometer (Orbiter 922; GN Otometrics, Copenhagen, Denmark) and headphones (TDH-39P; Telephonics, New York, USA), data was obtained using an ascending-descending technique, in 5 dB steps at all frequencies. If a participant made two or more responses to a set of three stimuli, she/he was deemed to have heard the sound.
Tinnitogram
The tinnitogram included pitch matching and loudness matching. The pitch-matching test started by presenting a pure tone at a frequency well below the perceived tinnitus pitch. Tones of different frequencies were then presented in octave intervals to gradually approach and identify the octave frequency that was closest to the perceived tinnitus pitch. Interoctave tones were then presented to more closely identify the tinnitus frequency. The pitch-matched tone was then compared with tones one octave higher and one octave lower, to ensure that the patient had not made the common mistake of 'octave confusion'. Following a final pitch match, the threshold of the pitch-matched tone was obtained to the closest 1-dB. The tone was then raised in 1-dB steps to determine the loudness match at the pitch-match frequency.
Procedures
We compared mean pure-tone average, mean pure-tone threshold at each frequency, mean speech reception threshold and mean word recognition scores among 1) tinnitus-affected ears (n=60), 2) non-tinnitus ears (n=60) of 60 patients with unilateral tinnitus, and 3) normal ears (n=60) of 30 control subjects. To analyze differences in the GIN performance among the three ears, we compared the mean GIN thresholds and the mean percentage of correct answers. Psychometric functions for each gap duration and each ear in both tinnitus and control groups were calculated. We examined the correlation between each the GIN threshold and the percentage of correct responses and the following parameters: age, sex, duration of symptom, initial VAS of tinnitus loudness, initial THI score, pitch and loudness in tinnitogram, pure-tone average, speech reception threshold, and word recognition score.
Statistics
The paired t-test was used to compare hearing thresholds, the mean GIN thresholds, and the mean percentage of correct answers between tinnitus-affected ears and non-tinnitus ears of the patients. Between-group comparisons of each audiometric data and the GIN results were performed by the Mann-Whitney U test. We analyzed correlations between variable factors and the GIN performance using multiple regression analysis. Commercial software (Windows SPSS, version 12.0, SPSS Inc., Chicago, IL, USA) was used for all data analysis in the study, and p<0.05 was considered to indicate statistical significance. Data are given as mean┬▒standard deviation (SD).
Results
Patient characteristics
In 60 patients with unilateral tinnitus, tinnitus occurred on the right side in 27 and on the left in 33. The mean duration of tinnitus was 31.2┬▒43.8 months, ranged 1-360 months. The mean VAS of tinnitus loudness at initial visit was 4.8┬▒2.6 and the mean THI score was 29.6┬▒24.0 on questionnaires. Mean pure-tone average for the tinnitus and control groups were 14.6┬▒11.2 dB HL (tinnitus-affected ears) and 15.1┬▒11.5 dB HL (non-tinnitus ears), and 9.4┬▒3.6 dB HL (right normal ears) and 9.7┬▒4.7 dB HL (left normal ears), respectively; there were significant differences of mean pure-tone thresholds at all frequencies between tinnitus-affected ears of the patients and normal ears of control subjects (Table 1). No significant difference of mean pure-tone average was found between tinnitus and non-tinnitus side of the tinnitus patients. Mean speech reception thresholds were 12.5┬▒10.9 dB HL, 12.8┬▒12.1 dB HL, and 8.8┬▒4.2 dB HL in tinnitus ears, non-tinnitus ears, and normal ears. Mean word recognition scores were 97.7┬▒6.0%, 97.5┬▒7.1%, and 96.8┬▒3.7% in tinnitus-affected ears, non-tinnitus ears, and control ears. As measured by tinnitogram, mean frequency was 3.3┬▒2.7 kHz and mean loudness was 5.2┬▒3.7 dB in tinnitus group. The most common matched pitch of tinnitus was 4 kHz (n=15), followed in descending order by 8 kHz (n=12), 0.25 kHz (n=11), 2 kHz (n=9), 3 kHz (n=5), 1 kHz (n=5), 0.5 kHz (n=2), and 6 kHz (n=1). The most common matched loudness of tinnitus was 5 dB SL (n=32), followed in descending order by 3 dB SL (n=9) (Table 1).
The GIN threshold and percentage of correct answers
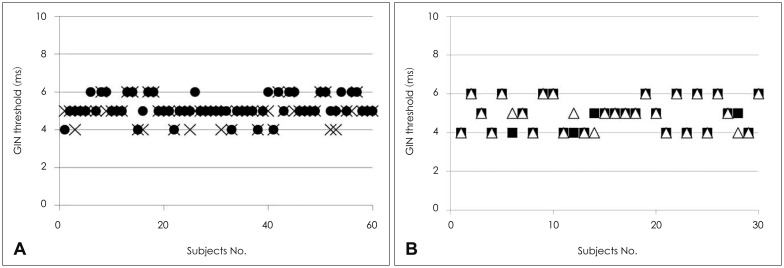
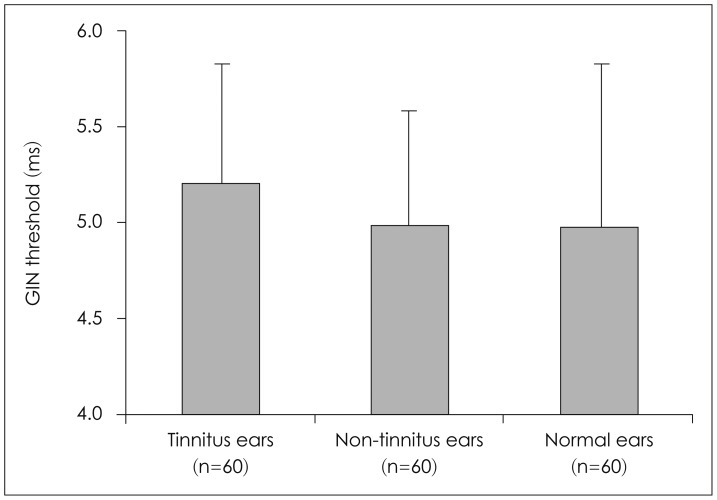
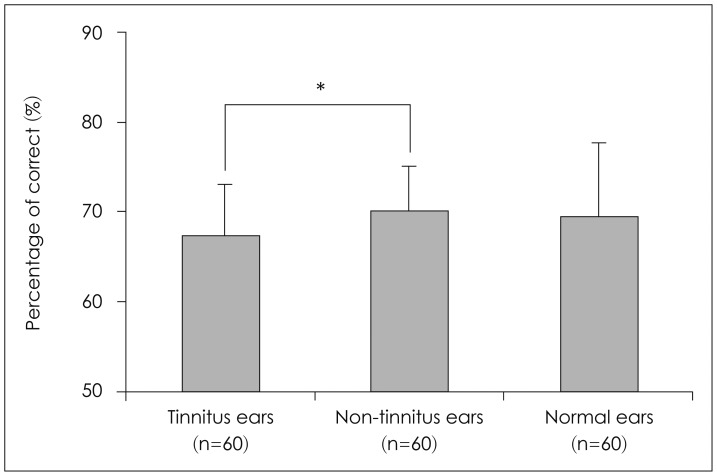
Individual GIN thresholds for both tinnitus and normal groups of subjects are shown in Fig. 2. There was no significant difference of distribution of the GIN thresholds between the tinnitus group and the control group. Among total 60 cases with unilateral tinnitus, 46 (76.7%) had the same GIN threshold in tinnitus-affected ears and non-tinnitus ears. The GIN threshold of 13 patients in tinnitus side was higher than that in non-tinnitus side, and only one showed lower threshold in tinnitus ear as compared with non-tinnitus ear. In 30 subjects with normal hearing, 26 (86.7%) had the same GIN threshold in left and right ears. The GIN threshold of 2 participants in left side was higher than that in right side, and the other 2 had lower threshold in left ear as compared to right ears. There was no significant difference of the average of the GIN thresholds among tinnitus ears (5.18┬▒0.6 ms), non-tinnitus ears (4.98┬▒0.6 ms) and normal ears (4.97┬▒0.8 ms) (Fig. 3). The mean GIN percentage of correct responses in tinnitus side (67.3┬▒5.5%) was slightly lower than that in non-tinnitus side (70.0┬▒5.5%) (p<0.05) but it was not significantly different from that in normal ears (69.4┬▒7.5%) (Fig. 4). There was no significant difference of the mean GIN percentage of correct answers between non-tinnitus ears in the tinnitus group and normal ears in the control group.
Psychometric function by gap duration
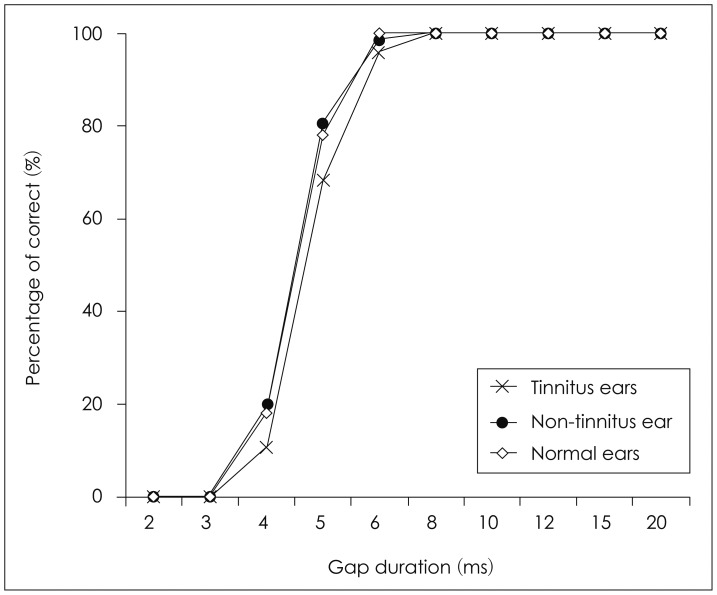
The analysis of psychometric function by gap duration was based on the quantity of total correct answers per gap duration for all the test lists. The correct responses for each specific test list were not considered. The overall GIN percentages of correct identifications in both ears among all of the subjects are presented, by gap duration, in Fig. 5. As there were 6 segments in all gap durations and 60 tested ears in each side, the percentages of correct was calculated from the following formula in this psychometric function curve: (total number of gaps identified/total number of gaps in each side, i.e., 360)├Ś100 (%). The mean percentage of correct answers for the 2-ms and 3-ms gaps was 0%. For the 4-ms gap, this percentage was approximately 11% (38/360) in tinnitus ears, 20% (72/360) in non-tinnitus ears, and 18% (66/360) in normal controls. At 5 ms, the percentage of correct responses increased considerably, reaching 68%, 81%, and 78% in tinnitus, non-tinnitus, and normal ears. At 6 ms, the percentage of correct was 96% for tinnitus side, 98% for non-tinnitus side, and 100% for normal group. For every gap equal to or longer than 8 ms, the GIN percentage of correct reached 100%. There was a trend of lower percentages of correct of 4 and 5 ms in tinnitus-affected ears than in non-tinnitus ears, but there was no significant difference of overall psychometric function between the tinnitus and control group.
Relationships between the GIN performance & parameters in tinnitus ears
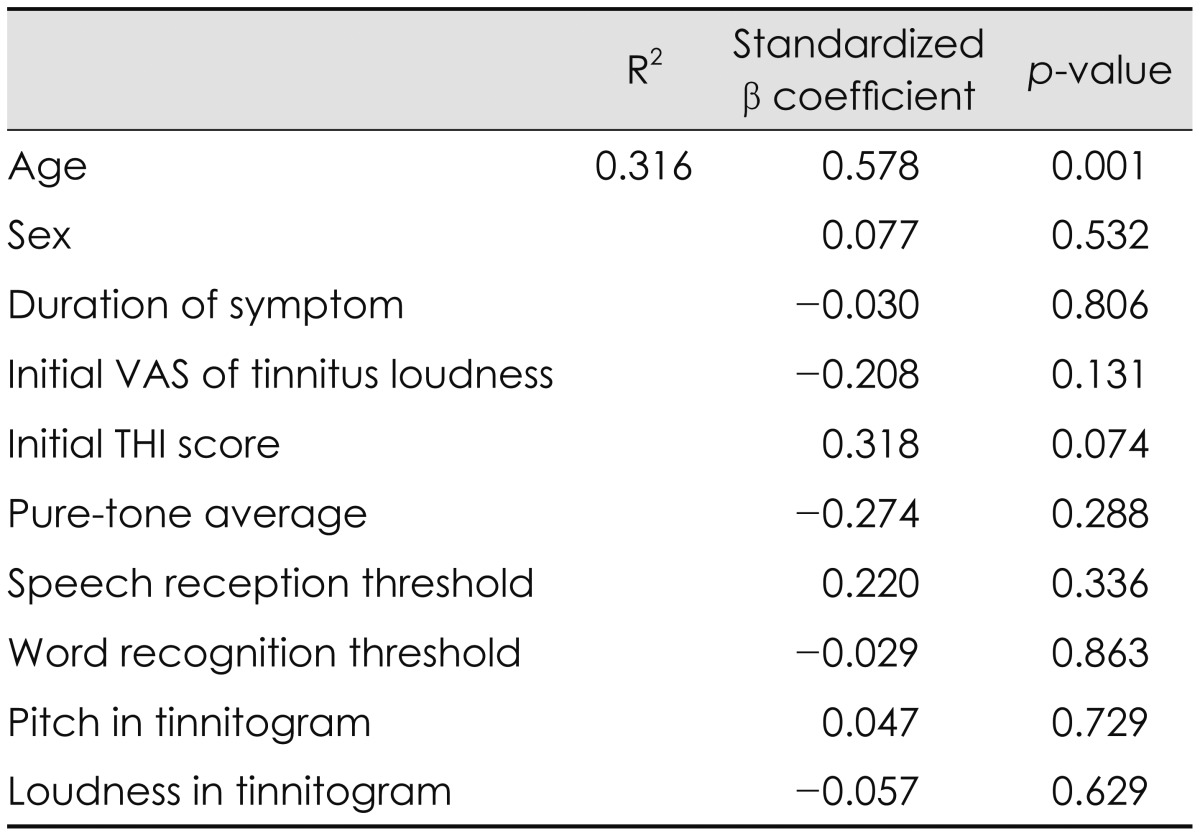
There was no significant correlation between the GIN thresholds and various factors including sex, duration of symptom, initial VAS of tinnitus loudness, initial THI score, pitch and loudness in tinnitogram, pure-tone average, speech reception threshold, and word recognition threshold in 60 tinnitus ears (Table 2). There was no significant correlation between the percentage of correct answers and these factors (Table 3). Age only showed a significant correlation with the GIN performance.
Discussion
The present study investigated the ability of the GIN test7) to differentiate a group of patients with unilateral tinnitus who showed symmetric hearing from a group of adults composed of normal hearing. Because hearing asymmetry would have main effects on the auditory temporal resolution,4,14,15) we enrolled patients with audiometrically documented symmetric hearing. Good performance in auditory temporal resolution requires precise neuronal firing with the balance of the excitatory and inhibitory synapses, which can be impaired in individuals with tinnitus and/or hearing loss. We hypothesized that tinnitus "fills in" the silent intervals in the background noise and that subjects with tinnitus show lower increased GD thresholds or the GIN performance. Contrary to our expectations, the two study groups did not perform significantly different from each other on both GIN test measures, which were supported by both the statistical and clinical analyses. The findings of the present investigation are not consistent with results from other investigations that reported auditory temporal processing deficits in individuals (hearing threshold Ōēż25 dB HL) with tinnitus.11,12) In these studies, they conducted the GIN test in 13 subjects with bilateral tinnitus and 7 with unilateral tinnitus, and they did not consider the laterality of tinnitus. This might provide a clue to the discrepancy in the GIN thresholds and percentages of correct identifications among patients with tinnitus. Further studies are required for application of the GIN test to patients with bilateral tinnitus and controls with matched hearing level.
The GIN test is known to be sensitive in confirming the central auditory processing disorders, being even more sensitive for structural damage or functional deficits in the central nervous system.7,16) In the present study, no difference between the two groups in the performance on the GIN test indicates that central auditory nervous system dysfunction is not clear in patients with unilateral tinnitus, although some studies have shown a relationship between central auditory pathway disorders and the perception of tinnitus.12,17) Someone may criticize that we did not recruit sufficient subjects with severe tinnitus. The mean of initial VAS of tinnitus loudness was 4.8┬▒2.6, and the mean of initial THI score was 29.6┬▒24.0 in our 60 patients who completed tinnitus questionnaires and hearing tests. In the present study, fourteen had initial VAS of 7 or more, nine had initial severe handicap of THI Ōēź58,18) and four had both of them simultaneously. Even though small number of patients with severe tinnitus, there was no significant difference of the GIN performance between nineteen cases with VAS of tinnitus loudness Ōēź7 or THI Ōēź58 and normal subjects. The mean pure-tone average of tinnitus group in this study were 14.6┬▒11.2 dB HL in tinnitus-affected ears and 15.1┬▒11.5 dB HL in non-tinnitus ears. The hearing thresholds of tinnitus ears were 22.3┬▒22.0 dB HL in 4 kHz and 28.4┬▒24.8 dB HL in 8 kHz (Table 1). Our findings suggest such a subtle cochlear damage could not affect temporal resolution in tinnitus, especially when pure-tone thresholds as conventionally measured appear normal or near-normal.
The mean thresholds for identification of silence gaps and the mean percentage of correct responses found were 4.97┬▒0.8 ms and 69.4┬▒7.5% for our 120 normal ears. In the literature on normal subjects, the mean GIN thresholds of 4.2-5.7 ms and the mean percentage of correct answers of 69-78% had been found.7,8,9,10,11,12,16) The results obtained in our control group were approximated to those found in the literature, more specifically to studies of Musiek, et al.7) and Shinn, et al.10) In consideration of means┬▒2SD as clinically normative values, normal limitations of the GIN performance were 6.57 ms and 54.4% for the present study. From the composition of total 60 gaps with 2, 3, 4, 5, 6, 8, 10, 12, 15, and 20 ms, the GIN threshold Ōēż6 ms and the percentage of correct Ōēź55% would be considered as normal in our individuals. Neither tinnitus-affected ears nor non-tinnitus ears in 60 patients with unilateral tinnitus showed abnormal GIN test measures, and this result imply that unilateral tinnitus has little influences upon auditory temporal resolution. On account of mild hearing loss in our tinnitus group, it is necessary to perform the GIN test in patients with unilateral tinnitus and moderate-to-severe hearing loss. Some clinical trials revealed adverse effects of hearing impairment on the GIN performance,15,19) however they directly compared hearing-impaired adults and normal listeners. If the GIN parameters correlate with the degree of hearing disturbance and have no relationship with the presence of tinnitus in patients with hearing loss, decreased temporal resolution in those seems to be more related to the level of hearing than to tinnitus itself.
Auditory temporal discrimination can be assessed utilizing a variety of methodologies by determining the GD threshold and the TMTF.3,5,6,7) There are obvious differences between the GIN test and traditional GD test. First of all, the GIN test uses white noise that contains every frequency within the range of human hearing (generally from 20 Hz to 20 kHz) in equal amounts.7) Using many different stimuli such as narrowband noise or broadband noise, the GD test has not been administered widely for clinical applications though researchers have shown this procedure to be valuable in measuring temporal resolution abilities. The reason for this lack of clinical GD testing is that traditional GD procedures are not suitable in a practical setting because they are time-consuming, making them difficult to use within a test battery and with subjects who cannot tolerate long periods of testing.7,16) The present investigation is relevant to previous studies that the GIN test is a clinically useful tool for evaluating GD abilities in adults with or without tinnitus.11,12) Both temporal discrimination and loudness perception may have a relation to the GIN performance, since noise gap means temporary absence of sound in time and intensity domain simultaneously. Nevertheless, TMTF measures are consistent with estimates of temporal acuity based on gap detection threshold20) and thus the GIN test is still one of important ways to assess auditory temporal resolution.
Analysis of the correlation of various factors to the indices of the GIN test demonstrated that age as the most significant and sole variable correlating with the GIN threshold and the percentage of correct identifications. It has been suggested that age has effects on the GIN performance and may affect test analysis and interpretation with published normative data.14,15,19) The strongest predictor of decreases in the GIN performance was increased hearing impairment, but a considerable independent influence of age was also documented. Interestingly, the average of the GIN threshold in older adults with essentially normal hearing is significantly higher than that in young adults with normal hearing.19) These results indicate that aging of the auditory system affects temporal processing, which affects the ability to hear subtle acoustic changes in a speech signal. This could be particularly true in the presence of background noise, where the fluctuations in the noise obscure the perception of the speech signal. In the present study, age had a good correlation with the GIN performance in the tinnitus group as well as in the normal control, even if data of the control group were not shown.
Conclusion
The GIN threshold of tinnitus-affected ears is not significantly different from that of non-tinnitus ears in patients with unilateral tinnitus who had symmetric hearing ability. There is no significant difference of the GIN performance between tinnitus patients and normal subjects. In our study population, age affects the GIN threshold and the percentage of correct answers. These findings suggest that tinnitus may not simply fill in the silent gaps in the background noise and not interfere in the ability of auditory temporal resolution.