A Case of Giant Osteoma Developed from the Mastoid Cortical Bone
Article information
Abstract
An osteoma of the temporal bone is a rare benign tumor. External auditory canal is the most common site of osteomas arising from temporal bone, and mastoid osteoma is very rare. A case of a 42-year-old female with a huge osteoma which developed from mastoid cortical bone is presented and the review of the temporal bone osteomas is discussed. The patient showed a huge and hard mass in the right mastoid area growing over a 20-year period. A temporal bone computed tomography scan demonstrated 2.3×2.3×4.3 cm sized bony tumor on surface of the right mastoid and squama. The resection of whole bony tumor with mastoid cortical bone was performed using retroauricular approach. Pathologic evaluation revealed the osteoma. The huge osteoma in the mastoid area may induce a cosmetic deformity. Early diagnosis and surgical removal of the osteoma may ensure an easy and complete treatment. The total resection of bony tumor including mastoid cortical bone is recommended to avoid recurrence.
Introduction
The osteoma is a mesenchymal osteoblastic tumor composed by a well differentiated mature osseous tissue with a predominant laminar structure.1) It has a benign nature with slow growth capacity.2) Usually most otolaryngologists encounter this disease as a radio-opaque lesion arising from within the fronto-ethmoid area.3,4) Osteoma of the temporal bone occurs rarely, and when this occurs, it is seen in the external auditory canal most commonly and mastoid osteoma is even more infrequent.4) Mastoid osteomas are usually asymptomatic and present as cosmetic deformity such as external mass or and auricular protrusion.3)
In this report, we present a case of a 42-year-old female with right huge retroauricular mass who was diagnosed with mastoid osteoma postoperatively.
Case Report
A 42-year-old woman visited out-patient clinic complaining of right retroauricular mass. The lesion of the right mastoid area developing over a 20-year period showed a severe cosmetic deformity (Fig. 1). On physical examination, both tympanic membranes were intact and huge, firm, painless, mass-like lesion was found on the right retroauricular area. Temporal bone computed tomography scan (TBCT) demonstrated 2.3×2.3×4.3 cm sized bony mass with a wide base on the surface of the mastoid cortical bone and squama without abnormalities of the middle and inner ear structures (Fig. 2).

Preoperative finding of right retroauricular mass. About 2.5×3.0 cm sized retroauricular bulging mass.
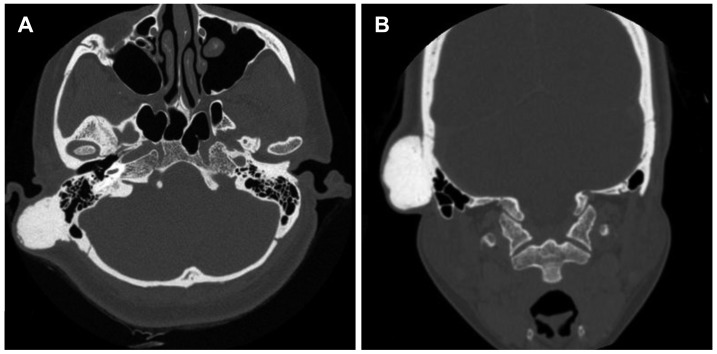
Preoperative finding in high resolution temporal bone computed tomography. A 2.3×2.3×4.3 cm sized, wide based, large mass with osteoid matrix is seen in right retroauricular area. A: Axial view. B: Coronal view.
The resection of tumor was performed using retroauricular approach (Fig. 3). The mass was widely exposed after elevation of mastoid periosteal flap and the margin of the mass was drilled down until the normal air cells were encountered. The mass attached to the lower part of the squama was drilled out. Remaining main mass was totally removed and the defect of mastoid area was reinforced by covering with the titanium mesh. The final histopathologic examination confirmed the osteoma with a compact subtype (Fig. 4). Four months after surgery, the surgical wound was intact, and the evidence of complication or recurrence was not found.

Intraoperative findings. A: Periosteum covering bony mass was elevated. B: Lateral aspect of the tumor was exposed. C: Posterior margin of the tumor was drilled down (arrowheads). D: Mastoid air cells were partially exposed (arrows).
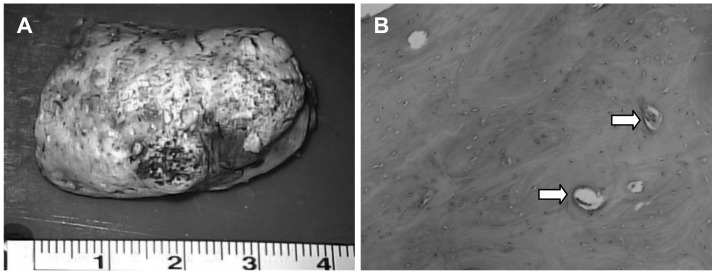
Gross specimen of the bony tumor (A) and pathologic finding (B). Dense sclerotic lamellae with organized Harvesian canals (arrows) were present.
Discussion
Mastoid osteoma is defined as a benign, circumscribed, slow growing tumor of the mastoid bone.5) Since the first publication of mastoid osteoma in the literature by Adam Politzer in 1887, there have been few case reports of osteoma occurring at temporal bone.3,6) Some authors have found 100 case reports regarding mastoid osteoma in the world literature in 1997 and added their 2 cases.7) Mastoid osteoma, one of the rare benign tumor attached to the cortex of the mastoid bone, has occurrence of 0.1% to 1% of all benign tumors of the cranial bone.1)
Osteomas have been reported in all parts of the temporal bone including the squama, mastoid, middle ear, glenoid fossa, Eustachian tube, styloid process, and both internal and external auditory canals.2) Among them, the external auditory canal is the most common location of osteomas in the temporal bone, followed by the mastoid and temporal squama.8) Middle ear osteomas are more common in males, whereas osteomas involving the temporal bone occur most commonly in females.2)
Osteomas are composed of well differentiated, mature bone and characterized by dense lamellae with organized Haversian canals histologically. The intratrabecular stroma contains osteoblasts, fibroblasts, and giant cells without hematopoietic cells. Histologically, there are three different subtypes: compact, spongiotic, and mixed. Compact osteoma has Haversian system, and has a dense, sclerotic, and round shape so that it is called ivory osteoma.4) It usually attaches to the mastoid cortex by pedicle or wide base. Spongiotic osteoma has spongiotic trabecular bone and fibrous cellular tissue such as marrow and this type is known as cancellous or osteoid osteoma.4) Slow growing compact osteomas are more common and have a wider base, whereas relatively faster growing spongiotic osteomas are rarely found and more likely to be pedunculated. Mixed osteoma is a mixture of compact and spongiotic osteomas. In the pathologic review of our case, the compact osteoma with well formed Haversian canals was observed.
Osteoma is thought to be originated from pre-osseous connective tissue and grows in response to irritants.2) Various etiologies including trauma, surgery, radiotherapy, chronic infection, and pituitary gland dysfunction have been proposed.9) However, any specific etiology was not identified in the present case.
Clinically most osteomas grow slowly and show benign features. They are usually asymptomatic and may be stable for many years. When occurring in the squamous or mastoid portion of the temporal bone, they may present cosmetic deformities such as external bulging of the mass or auricular protrusion. Rarely, pressure-induced pain can be referred to the neck, auricle, or middle ear, and when meatal obstruction occurs, conductive hearing loss or chronic suppuration may be produced.3) Although the size of the tumor at the time of presentation may be various, it is usually smaller than 3 cm.10) The present case presents a huge mastoid osteoma that the maximal diameter exceeds 4 cm without any pain or other symptoms.
TBCT scan is the most efficient diagnostic tool in the mastoid osteomas as well as in osteoma of other area. The osteoma can be demonstrated as a high opacity, well-demarcated, dense outgrowth of sclerotic lesion from the mastoid bone by TBCT scan.1) Differential diagnosis of osteoma includes other benign bone-forming lesions such as osteoid osteoma, benign osteoblastoma, ossifying fibroma, fibrous dysplasia, chondroma, osteochondroma, calcified meningioma, isolated eosinophilic granuloma, Paget's disease, and giant cell tumor. Also, malignant lesions such as osteosarcoma and osteoblastic metastasis should be considered. The differential characteristic of these diseases from the osteoma is that radiologic borders of these other lesions are less clear than those of osteomas.11)
The treatment of choice for mastoid osteoma is a surgical resection. When the lesion is small and asymptomatic, it is possible to follow up patients with a regular radiologic imaging. However, if there is a constant pain, neurological alterations, or evidences of other complications, the surgical removal is indicated. Surgical removal of osteoma of the mastoid and squamous portion for the purpose of the cosmetic improvement is not usually indicated. As presented in the present case, very huge osteomas in the area need to be removed. In the surgical point of view, it is essential to excise the lesion completely until normal mastoid air cells are exposed. If complete removal is possible, recurrence rate is very low.12,13) In mastoid osteoma extending into the facial nerve, bony labyrinth, and fallopian canals, complete excision is not indicated and partial removal is possible because damage to these structures is likely.2,4) Facial nerve injury, tearing of the sigmoid sinus, and postoperative auricular discharge have been reported as complications of the surgery.13)
The reconstruction of the mastoid cortex defect using titanium mesh after mastoidectomy has been previously reported.14) The reconstruction is emphasized to prevent a cosmetic deformity in the postauricular area and also to maintain an aerated mastoid cavity.14) Usually, mastoid cavity formed after intact-canal-wall mastoidectomy is reconstructed using periosteal flap repositioning. However, in cases of a large mastoidectomy, periosteal flap repositioning alone can result in some dimpling in the postauricular area.15) Thus, when posterior canal wall with a periosteal pocket is present and large mastoidectomy is performed, functional reconstruction of the mastoid cortex with titanium mesh can be considered. In this case, because the tumor had a broad based-attachement to the mastoid cortex, which resulted in wide resection of the mastoid cortex, there was a possibility that periosteal flap repositioning alone may induce a dimpling in the postauricular area. Therefore, the mastoid cortex reconstruction using titanium mesh was planned in this case.
The prognosis of the mastoid osteoma may be considered to be good in cosmetic and curative aspects when it is completely excised. Malignant transformation has not been reported in the medical literature.13) Although the recurrence was rarely reported in the mastoid osteoma cases, there were 2 cases with recurrence after treatment.9)
Acknowledgments
This study was supported by a clinical research grant provided by Seoul National University Boramae Medical Center.