Conductive and Mixed Hearing Losses: A Comparison between Summer and Autumn
Article information
Abstract
Background and Objectives
Conductive hearing loss is common among children and adults. This study aims at comparing the results of conductive hearing loss in summer and autumn.
Subjects and Methods
Puretone audiometry and tympanometry tests were done for all patients who referred to the Iranian-based audiology center of Imam Khomeini Hospital in Ahvaz. Data on the patients with conductive or mixed hearing loss were analyzed. The impacts of season, age, and etiology of the disease were analyzed on the patients who visited the audiology clinic due to the conductive hearing loss in summer and autumn.
Results
One hundred and fifty nine patients in summer and 123 patients in autumn had conductive or mixed hearing loss. Their age ranged from four to 82 years, with the average age of 35. The percentage of the patients, with acute otitis media and chronic otitis media (COM), who visited this clinic, was significantly higher than those with middle ear problems. COM and mastoid surgeries rate was higher in summer than autumn among adults.
Conclusions
There is no relationship between season and middle ear diseases between children and juveniles, but COM and mastoid problems are more common in summer among adults visiting this clinic. Most of the patients had mild conductive hearing loss and bilateral middle ear impairments.
Introduction
One type of hearing loss is conductive hearing loss (CHL) that shows an air-bone gap in the standard audiometry.1) The sound is affected before entering the inner ear in CHL2) and leads to some undesirable consequences. The acquired unilateral CHL reduces the ability to localize sound3) and the affected individuals' life quality.4) Moderate or even mild hearing loss could be a significant problem for school children5) because educational listening is not easy in the presence of background noise.2) Furthermore, a mild hearing loss in children may cause impairments in the development of communication, behavioral skills,6) learning ability,7) and speech.8) Eustachian tube dysfunction,9) ossicular chain problems caused by head trauma10) and otitis media (OM) are factors that may lead to CHL. The most common consequence of OM is the hearing impairment,11) and there are 29 types of OM.12) Although according to some studies the CHL caused by otitis media can lead to secondary problems such as auditory processing disorder,2) cognitive, language, speech and behavior problems,13) there is no strong evidence on the impact of the middle ear effusion on speech and language, so this subject is a matter of controversy.11) Allergies and environmental factors (seasonality and upper respiratory infections) may also lead to OM. In some studies, OM was more commonly observed during the autumn and winter as against the summer in both northern and southern hemispheres.14) According to a prospective, longitudinal cohort study in Southern Brazil on 156 children in autumn, winter and spring, using tympanomrtry and otoscopy, the incidence of serous otitis media was higher in winter, especially, among children of lower socioeconomic classes.15) A retrospective study on 340 infants below 2 years old with recurrent acute otitis media (RAOM), conducted by Cairo University Hospital from May 2011 to April 2012 indicated that winter is an important factor that may cause RAOM.16) In 2012, Ting, et al.,17) carried out a multiple database study in Taiwan and reported acute otitis media (AOM) as a prevalent OM among children in spring. A higher resolution rate in summer and a lower resolution rate in autumn were reported by Gordon, et al.18) prospective study in New York. They monitored the children who were referred to a tertiary medical center over 3 years. There was a positive correlation between resolution rates and average daily temperatures. otitis media with effusion (OME) could change the middle ear morphologically; particularly in the pars tensa.19) Gram negative bacteria such as pseudomonas can cause chronic suppurative otitis media that is more common in developing countries and in poorer areas of the developed world.20) Reviewing the audiograms of 164 citizens of Ankara, Turkey, with idiopathic sudden sensory neural hearing loss (ISSHL) over 5 years indicated that ISSHL was more profound in autumn than in summer. Also hearing loss was more profound in winter as against summer and spring. Therefore, the seasonal variation of hearing loss level of ISSHL was more profound in winter.21) Considering the seasonality as a risk factor for OM,22) incidence of conductive hearing loss is varied in different seasons because warmth affects the enteric bacteria colonization of chronic suppurative otitis media, and the frequency of isolation of enteric bacteria rises in hot climates.23) When relative humidity rises up to 80 percent, incidence of otomycosis infection goes higher, and it infects middle and external ears.24) Dampness is also the most important environmental factor connected with ear infection, since molds have serious effects on humans' immune system.25)
Several tests can be used to examine ear problems. One of these tests is tympanometry with a high degree of specificity and sensitivity that can diagnose the problems of the middle ear. Additionally, it is an objective and reliable technique. Likewise, el-Sayed and Zakzouk26) used tympanometry to determine the prevalence of secretory otitis media.
This study aims at determining and comparing the prevalence of conductive and mixed hearing losses in both summer and autumn among children, juveniles and adults who referred to the Iranian-based audiology center of Imam Khomeini Hospital, in the city of Ahvaz.
Subjects and Methods
This is a descriptive study of all patients referred to the audiology center of Imam Khomeini Hospital, in the city of Ahvaz, Iran. Otoscopy, puretone audiometry, tympanometry and acoustic reflex tests were done on all patients. However, children under four years old who could not cooperate with the audiometry test were excluded from this study. Only the results connected with those patients, who at least one of their ears had conductive or mixed hearing loss, were analyzed. The results are shown in two parts of descriptive and inferential statistics. Descriptive statistics such as frequency distribution for the first part and the chi-square test for the second part were used for the analysis.
Results
One hundred and eighty seven patients in summer and 133 patients in the autumn had conductive or mixed hearing loss. Both ears of a total of 320 patients were evaluated. Thirty eight persons had traumatic CHL, so they were excluded from the study because this condition is not related to seasonal variation. The results related to 282 patients were analyzed. Their ages ranged from 4 to 82 years with an average of 35.09±18.87. Thirty seven (13.12%) of them were children (<12 years old), 24 (8.51%) were juveniles (12-18 years old), and 221 (78.36%) were adults (>18 years old). The box plot of age in two seasons is seen in Fig. 1. Seventy four patients (26.2%) had unilateral and 208 (73.8%) had bilateral middle ear impairments. Patients' sex and types of hearing loss are shown in Table 1, 2, respectively. CHL was the most common type of hearing loss in two seasons, and there is no significant relationship between the type of hearing loss and season; neither in the right ear nor in the left (Table 2). Mild hearing loss was observed more frequently than other types. Tympanometry results and degrees of hearing loss are shown in Table 3, in detail. The percentage of patients with AOM and chronic otitis media (COM) visiting this clinic was significantly higher than OME, otosclerosis and mastoid surgeries (Table 4). To examine the relationship between the season and type of the disease, Fisher's exact test was done, yet no significant relationship was found between children and juveniles (Table 5, 6). However, COM and mastoid surgery were more frequent than others in summer, and unknown problems were more common in autumn, among adults (Table 7). COM, mastoid surgery, otosclerosis and unknown diseases were more common among adults compared with children (p<0.05); especially, COM (p<0.001).
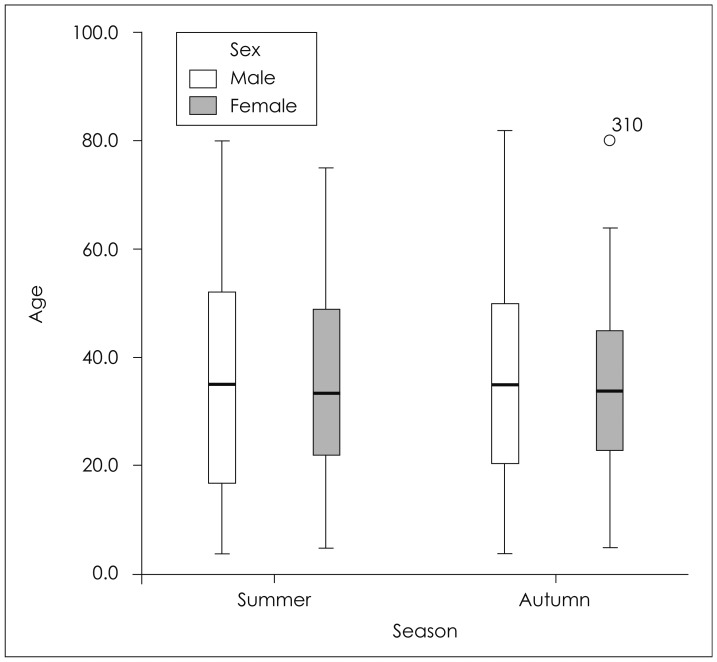
Box plot of age in summer and autumn.
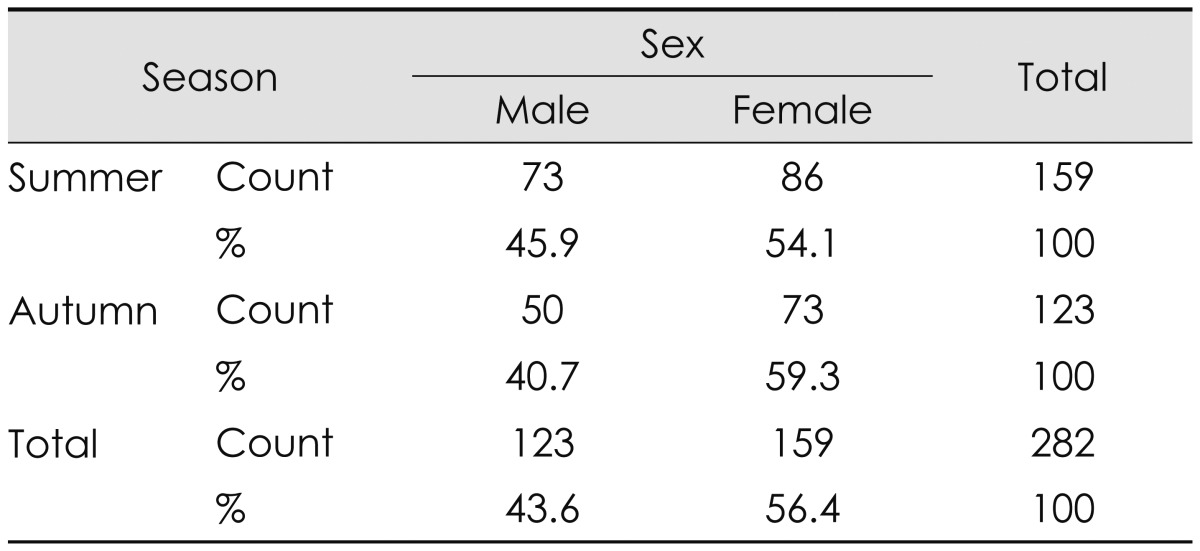
Sex of patients in summer and autumn
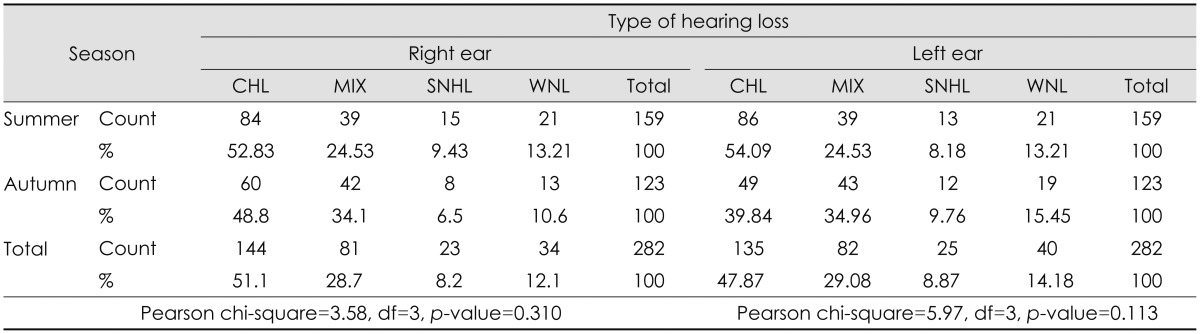
Type of hearing loss
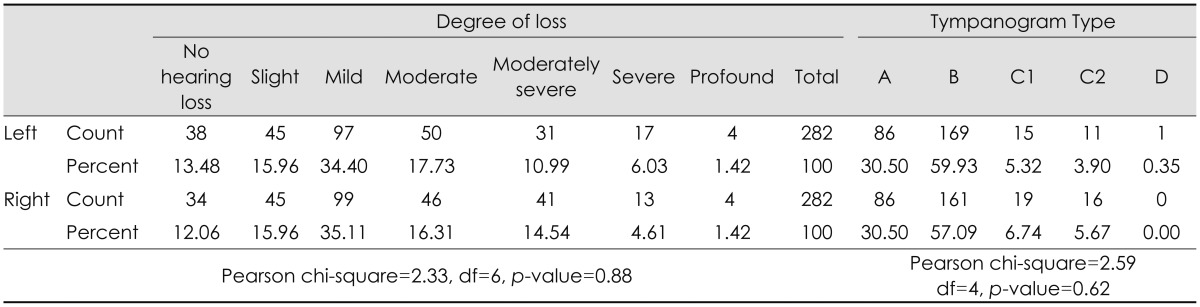
Degree of hearing loss and tympanometry results in 564 ears
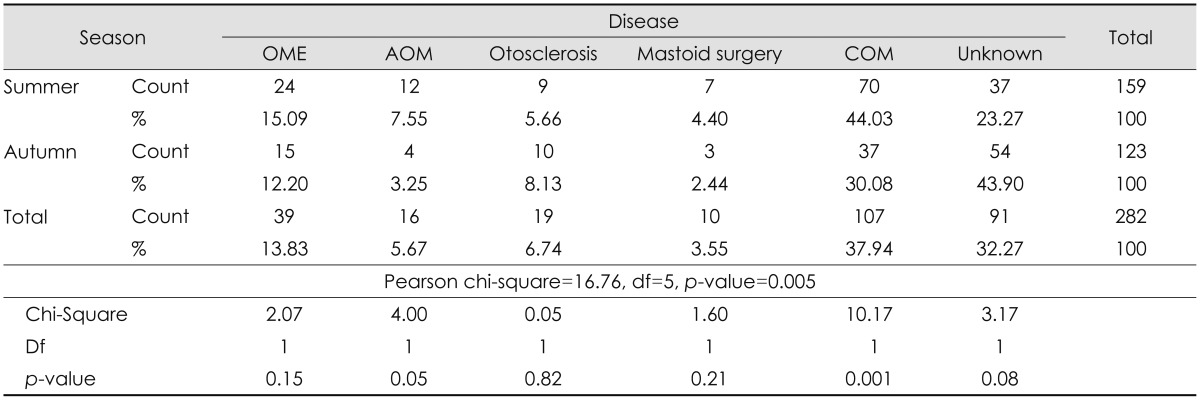
Diseases in patients
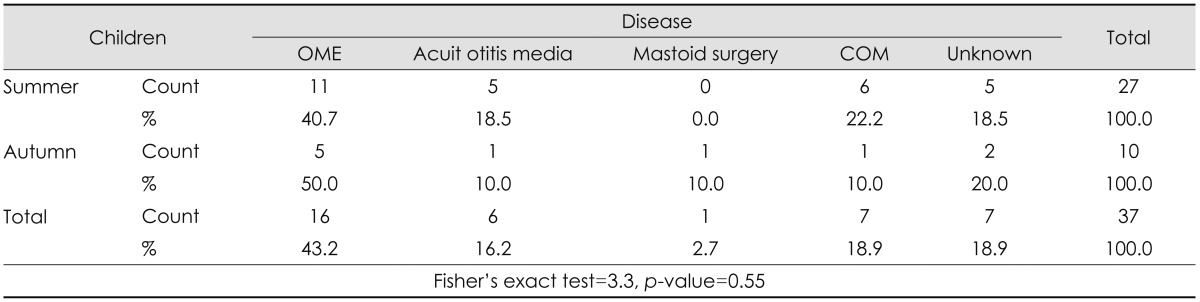
Diseases in children

Disease in juveniles
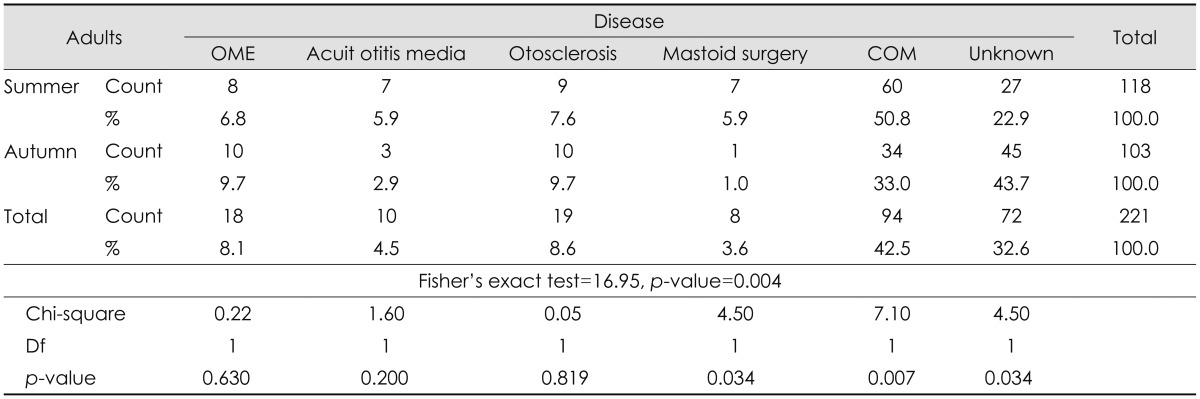
Disease in adults
Discussion
The middle ear problems are prevalent among people, and it has been shown in various studies that seasonality is an important factor. The present study was designed to find a difference in the prevalence of CHL with regard to the seasonal variation (especially summer and autumn). The results of this study showed that mastoid surgeries and COM are more common among adults, in summer. This may be resulted by the high temperature and humidity during summer in Ahvaz (temperatures rise above 50 degrees Celsius in summer). This finding is in harmony with Ibekwe, et al.'s27) findings that showed tympanic membrane perforation rate, as a common cause by suppurative otitis media, is significantly high in wet and humid seasons in Africa. Similarly, otorrhea, otalgia, tinnitus and itching were more prevalent in humid seasons than other ones. An unanticipated finding of this study was that there was no significant relationship between OM and season (p=0.55) among children, while previous studies have reported a strong relationship (Ting, et al.,17) Rovers, et al.,28) Castagno and Lavinsky,15) and Salah, et al.16)). This result may be due to the small number of children in the study.
Williams studied for six years (1998-2004) the audiometric results (otoscopy, 1000 & 4000 Hz audiometry, tympanometry and acoustic reflexes) of children from three urban primary schools in Perth, Australia (n=119). In 18 children (19.1 percent), mild or moderate hearing loss was diagnosed. Hearing loss in older children was less common (p=0.007) and had no relationship with season. Fifty children had chronic suppurative otitis media or OME in one or both ears [21 persons (17.6%) unilaterally and 29 persons (24.4%) bilaterally]. OME was seen in 22 of 119 patients (18.5%) [13 children (10.9%) bilaterally and 9 children (7.6%) unilaterally]. They concluded that there was insufficient evidence to prove any relationship between the middle ear diseases and season (p=0.52). They found no association between OME and age, either (p=0.22). Likewise, they found no association between OME and season (p=0.56).5) In the present study, like Williams's study, most hearing losses were bilateral, and no relationship between season and CHL was found among children.
El-Sayed and Zakzouk26) considered the type B tympanogramas as an indicator for secretory otitis media and investigated the point prevalence rate of the type B in a random sample of 4214 children. The type B tympanogram was seen in 5.7 percent of the sample unilaterally and 8.1 percent bilaterally. The type B prevalence in this population was related to season. Similarly in the present study, bilateral CHL was more common than unilateral CHL. El-Sayed found seasonal relevance for otitis media, while we did not find any significant relationship between season and otitis media among children. That might be because winter is different from other seasons. However, we compared autumn with summer, and winter is colder and dryer in which upper respiratory infections are more prevalent.
One of the limitations of this study was the using of data from only two seasons of the year, yet it is better to investigate all four seasons. It is also to suggest that further study be conducted with more focus on children. In addition, this study was not a population-based study and there may be a risk of selection bias.
Conclusion
According to the findings of this survey, in the audiology center of Imam Khomeini Hospital in Ahvaz, more patients with CHL visited the clinic in summer as against autumn. The most significant finding of this study is that there is no relationship between season and the middle ear diseases among children and juveniles, but COM and mastoid problems are more common in summer, among adults. As most of the patients had mild CHL, it may be useful to both clinicians and patients to know that more patients may complain about CHL in summer.
Acknowledgments
We acknowledge the Research Consultation Center (RCC) for providing technical assistance. We also appreciate Mr. Zargarshoushtari M., Ms. Mehran S., Ms. Bavarsad M. and Ms. Samadi S. for assisting with evaluating the patients.