Introduction
The ability to communicate effectively with others is made possible by an intact auditory mechanism. The importance of having a normal hearing is even more crucial for children who are in the process of developing their speech and language. Physiologically, both the peripheral and central auditory systems are involved in processing the auditory inputs. If the organs within the auditory system are disrupted, hearing loss occurs [1]. To limit the negative consequences of hearing loss, hearing assessments should be conducted as soon as possible so that those with hearing loss can undergo appropriate interventions in a timely manner [2,3]. In fact, hearing-impaired children who received early interventions demonstrated better speech improvements than those who received late interventions [1,3].
The auditory status of an individual can be determined using subjective or objective tests. Pure tone audiometry (PTA) is an example of a known subjective test for the diagnosis of hearing disorders [1]. In this test, the hearing levels at specific frequencies are obtained by asking the individual to behaviorally indicate his/her responses when specific sounds are presented. Nevertheless, objective tests are more appropriate when testing difficult-to-test children as their cooperation (in giving subjective responses) is not required.
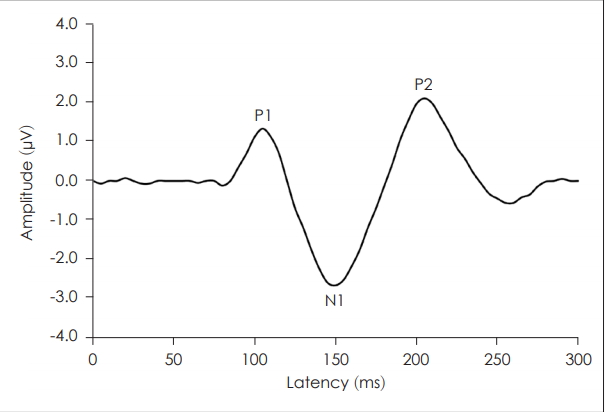
The cortical auditory evoked potential (CAEP) is a useful objective test to measure the function of auditory organs within the central auditory nervous system [1,4]. It is a component of the auditory evoked potential (AEP) classification based on its’ peak latencies [4]. The obligatory CAEP represents the neural detection of the evoking auditory stimuli and is characterized by a series of prominent peaks (P1, N1, and P2) typically occurring within 50-300 ms (Fig. 1).
To record the CAEP, scalp electrodes are placed on specific locations of the head and stimuli such as tone bursts or speech syllables are presented repetitively to evoke electrical potentials along the central auditory pathway. As reported elsewhere, CAEP has been found to be sensitive in identifying hearing loss and disorders affecting the central auditory pathway including tumors, multiple sclerosis, and brain injury [5-7]. Abnormal CAEP waveforms have also been reported in children with syndromic features, attention deficit hyperactivity disorder, autism, learning disabilities, auditory processing disorder, auditory neuropathy, and epilepsy [8-15].
Before a specific test can be applied in clinical settings, its normative data must be established. To our knowledge, normative CAEP data for Malaysian children have not been published. However, prior to the development of the normative data for the CAEP, the possible influence of fundamental variables such as age and type of stimulus on the CAEP should be studied. Therefore, the aim of the present study was to determine the effects of age and stimulus type on the CAEP waveforms. Subsequently, the normative CAEP data for Malaysian children would be established.
Subjects and Methods
Participants
In this study, which employed a repeated-measures design, thirty-five Malaysian children aged between 4 and 12 years (mean=8.4±2.7 years) were recruited. They were all healthy and had no hearing, speech, or learning disabilities (their PTA thresholds were less than 25 dB HL at frequencies of 0.25 to 8 kHz). The study procedure was approved by the Institutional Review Board (FF-108-200), which is in accordance with the 1975 Declaration of Helsinki and its later amendments. Prior to the data collection, written informed consent was obtained from the caregiver of each child.
Test equipment and procedures
A two-channel Biologic AEP device (version 6.2.0 by Natus Medical Inc., Pleasanton, CA, USA) was used to record the CAEP. The active electrode was placed on the earlobe, the indifference electrodes were placed on C3 and C4, and the reference electrode was placed on the forehead. These electrode sites were chosen to produce optimal CAEP waveforms [4]. To ensure good recording quality, the electrode impedance was maintained below 5 kΩ throughout the recording sessions.
During the testing, the children were seated comfortably facing a loud speaker positioned at a one meter distance at 0° azimuth. They were instructed to relax and minimize their body movements, while watching a voiceless movie of their choice. The CAEP waveforms were recorded using a 1 kHz tone burst and with the speech syllable /ba/ transmitted at an intensity level of 65 dB SPL. The tone burst was ramped using a Blackman filter with a 30-cycle rise/fall time and a 10-cycle plateau time. The speech syllable was custom built using a Sound Forge software (version 8.0 by Sony, New York City, NY, USA). The repetition rate for both stimuli was 1/s. The time window was set to 533 ms with 512 points. The waveforms were amplified 50,000 times and band-passed at 1-30 Hz. The artifact rejection level was set at 95 µv to eliminate movements and biological interference. Breaks were given between the sessions or as requested by the subjects.
Data analysis
The prominent peaks of the CAEP were identified and plotted by experienced researchers. The latencies and amplitudes of the P1, N1, and P2 peaks were computed for each subject. Since the data were found to be normally distributed (p>0.05 by Kolmogorov-Smirnov test), parametric analyses could be conducted. Pearson correlation analysis was used to determine the effect of age on the CAEP results. A paired t-test was employed to determine the influence of stimulus type on the CAEP waveforms. The statistical significance level was set at p<0.05. To support the hypothesis testing results, Cohen‘s effect size (d) was computed. The effect sizes were interpreted as small (d=0.20), medium (d=0.50), and large (d=0.80) [16]. All data were analyzed using the SPSS software version 20 (IBM Corp., Armonk, NY, USA).
Results
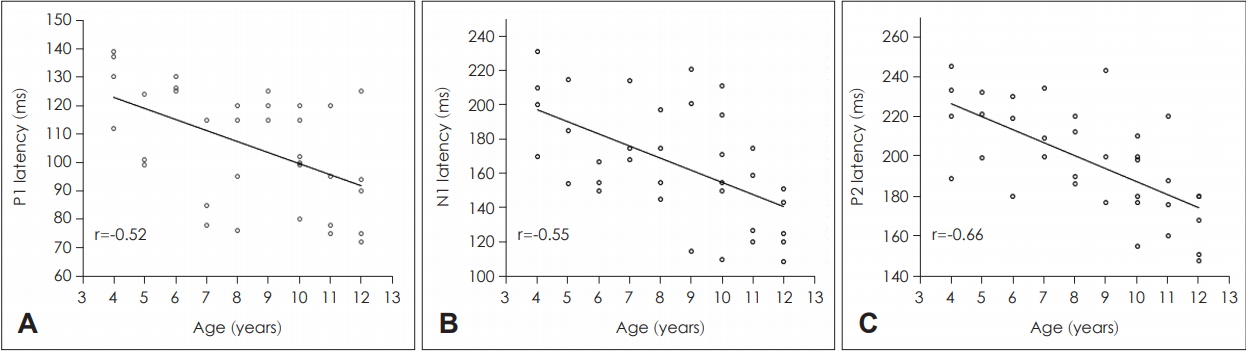
The CAEP waveforms were successfully recorded for all children. Based on the correlation analyses, no significant relationship was found between age and the CAEP amplitude at all peaks for both stimuli (p>0.05). Likewise, no significant correlations were found between age and tone-evoked CAEP latencies (p>0.05). In contrast, for the CAEP latencies recorded using the speech syllable /ba/, significant negative correlations were found between age and P1 (r=-0.52, p=0.001), N1 (r=-0.55, p=0.001), and P2 (r=-0.66, p<0.001). That is, all peak latencies shortened with age. The correlation plot for each of these peak latencies is illustrated in Fig. 2. To further verify the age effect on the CAEP waveforms, we compared the CAEP results between the following three age groups: Group 1 (4-6 years), Group 2 (7-9 years), and Group 3 (10-12 years). Consistent with the correlation analyses, one-way ANOVA found no significant differences in the CAEP amplitudes between the age groups for both tone and speech stimuli (p>0.05). The mean differences between the three age groups were also insignificant for the tone-evoked CAEP latencies (p>0.05). However, when evoked by speech stimuli, children in Group 3 revealed the shortest peak latencies (p<0.05). The longest peak latencies were noted for those in Group 1 (p<0.05). Based on the post-hoc analysis, significant differences in peak latencies were found between Group 1 (younger children) and Group 3 (older children) (p>0.05). Significant mean differences were found between Group 1 and Group 2 only for P1 (p<0.05) but not for N1 and P2 (p>0.05). When Group 2 and Group 3 were compared, significant results were noted for N1 and P2 (p<0.05). The latencies between Group 2 and Group 3 were found to be comparable to P1 (p>0.05). Collectively, these ANOVA results were all consistent with the correlation analyses supporting the notable age effect on speech-evoked CAEP latencies.
Table 1 reveals the mean and standard deviation for each peak latency when stimulated by the tone burst and speech stimuli. As shown, no significant difference in latency was found between the tone burst and speech syllable for all peaks (p>0.05). These insignificant p values were further supported by the small effect sizes (d<0.20). The corresponding CAEP amplitude analyses are shown in Table 2. As indicated, the speech syllable /ba/ produced a higher mean P1 amplitude than the 1 kHz tone burst (p=0.001) and the magnitude of difference was medium (d=0.74). For the other peaks, no significant difference in the CAEP amplitude was noted between the two stimuli (p>0.05).
Discussion
In the present study, the CAEP waveforms were recorded using tone burst and speech stimuli in Malaysian children. The CAEP latencies and amplitudes obtained are consistent with those of previous studies and are within the published ranges [4,17,18]. The P1, N1, and P2 peaks of the CAEP reflect the encoding of potentially detectable sound by the neurons of the auditory cortex [19,20].
As reported elsewhere, the CAEP waveforms reflect the maturation of the central auditory nervous system in their latency, amplitude, or morphology [21]. These maturational changes are complex and extend well into the second decade of life [22]. In this study, it was found that age was more related to the CAEP latencies than amplitudes, and these relationships were more predominant with the speech-evoked CAEP. Specifically, significant reductions were noted in speech-evoked P1, N1, and P2 latency. These findings are in line with previous studies where, generally, age related changes in the CAEP are associated with reduced latencies. For example, P1 latency has been reported to decline with age [22,23]. A similar pattern has also been found for N1 latency [23,24]. To obtain more insight into this age effect, the peak latencies were compared between the three age groups (i.e., 4-6, 7-9, and 10-12 years). As shown, the older children (aged≥7 years) demonstrated shorter peak latencies than younger children (aged 4-6 years), which is consistent with the existing literature [25]. However, conflicting findings have been reported for P2 latency. That is, while some studies revealed no age-related changes in P2 latency [26,27], others found a reduction in P2 latency with age [28]. Unlike the speechevoked CAEP outcomes, the present study revealed no significant association between age and the CAEP latencies recorded with the tone burst stimulus. This may indicate that the physiological detection of simple sounds, such as tones, could be processed with ease even in younger children.
As revealed, no significant effect of age was discovered on the CAEP amplitudes evoked by either stimulus. In the literature, contradictory findings have been reported regarding the maturational effect on the CAEP amplitudes. As such, N1 amplitude was reported to increase with age [24]. Consistent with the present study findings, no significant age effect on N1 amplitude was found in other studies [22,29].
In the present study, both simple (1 kHz tone burst) and complex (speech syllable /ba/) stimuli were used to record the CAEP. The tone burst was chosen as it is a standard stimulus available in the conventional two-channel AEP device. That is, the tone-evoked CAEP can be conveniently performed by audiologists and hearing clinicians as the AEP device is readily available in many hospitals or clinics. However, the speech-evoked CAEP was studied as the speech stimulus is more natural and contains multiple frequencies [4]. As such, different findings would be expected when the CAEP is recorded with two different stimuli. As revealed, the speech syllable /ba/ produced significantly higher P1 amplitudes than the tone burst. This finding is consistent with previous reports [4,21,30]. In a study by Ibrahim, et al. [30], the CAEP waveforms were recorded from 15 healthy Malay adults using tone burst and speech stimuli. In line with the present study outcomes, they found that the speech stimuli produced significantly larger P1 amplitudes than the tone burst [30].
However, the CAEP latencies recorded with both stimuli were found to be comparable. This finding is sensible as the CAEP amplitudes are typically more affected than the CAEP latencies when stimuli with different frequencies are used [4,25]. It is worth noting that even though no significant difference was found for the N1 amplitude between the two stimuli, the p value obtained was on the verge of significance (p=0.053). In this regard, if more children could be recruited, more accurate statistical results can be produced. Future research with larger sample sizes is warranted to verify this possibility.
While no significant effect of age was found on the toneevoked CAEP results, the CAEP latencies recorded with the speech syllable became shorter with age. Both tone-burst and speech stimuli were appropriate for recording the CAEP. However, significantly larger P1 amplitudes were found for the speech-evoked CAEP. The preliminary normative data for the CAEP provided in the present study may be beneficial for clinical and research applications involving Malaysian children. Nevertheless, future large-scale research is recommended to further support and validate the present study findings. As such, the sensitivity and specificity of the CAEP can be determined by testing Malaysian children with specific auditory disorders. Furthermore, these normative data can also be compared with the performance of hearing-impaired children who use hearing aids or have cochlear implants. These aspects of CAEP are subject to further research.