Objective Comparison of Benefits Derived From Contralateral Routing of Signal Hearing Aid and Bone Conduction Device in Noisy Surroundings in Patients With Single-Sided Deafness
Article information

Abstract
Background and Objectives
Single-sided deafness (SSD) leads to non-participation of the diseased ear in generating adequate auditory input, which results in poor speech discrimination in noisy surroundings. The present study objectively compared the audiological benefits rendered by contralateral routing of signal (CROS) hearing aid and bone conduction device (BCD) in patients with SSD >70 dB HL using the modified hearing in noise test (HINT).
Materials and Methods
Patients with SSD >70 dB HL in poor and clinically normal hearing in the better ear were enrolled. Patients aged <18 or >70 years, with a history of neurological insult or ear infection in the last 3 months, mental retardation, psychiatric or developmental disorders, and diabetes were excluded. Modified HINT was performed with the affected ear unaided, aided with CROS hearing aid, and with BCD, generating three groups. Noise signal was presented at a fixed intensity of 65 dB at the neutral position in the center and speech signal was presented to either ear sequentially. The test was repeated with the speech signal fixed at the neutral position and the noise signal presented to either ear.
Results
BCD led to a better signal-to-noise ratio (SNR) than CROS hearing aid in all situations except when noise was centralized and speech was presented to the affected ear.
Conclusions
A benefit was observed when auditory rehabilitation was used for the affected ear as demonstrated by better SNR scores. The results showed that BCD performed better than CROS hearing aid.
Introduction
Single-sided deafness (SSD) implies a state of one ear being normal with the contralateral ear being hearing impaired. This leads to non-participation of the diseased ear in generating adequate auditory input [1]. This induces 1) head shadow effect, which blunts the intensity of the sound signal which arises from the diseased ear’s side and, 2) squelch effect, which affects speech discrimination in noisy surroundings and 3) binaural summation-lack of this effect diminishes the loudness of sound signal. These effects negatively impact the quality of life in the absence of binaural hearing.
The conception that SSD does not constitute a disability [2] aggravates its impact on patient’s lifestyle and leads to delay in diagnosis and treatment. Rehabilitative devices enhance hearing by redirecting sounds from the non-functional ear to the better ear. Currently, contralateral routing of signal (CROS) and bone conduction devices (BCD) are the two core intervention methods for the treatment of SSD. Though these devices remove the head shadow effect by collecting sound from the impaired side, they fail to employ bilateral auditory integration [3]. Consequently, they have limited effect on sound localization [4] and speech perception with binaural summation [5]. Thus, while considering the advantageous effect of rehabilitative devices for unilateral hearing loss (UHL)/SSD, one should use outcomes that objectively evaluate monaural hearing. Our study compares the audiological benefits provided by CROS and BCD by measuring their ability to overcome the head diffraction and speech in noise effects in SSD individuals.
Materials and Methods
This cross-sectional study was conducted at our tertiary care centre (June 2015–November 2016) on outpatient basis after receiving approval from Institutional Ethics Committee (RT-22/23.06.2015). Patients with SSD with better ear pure tone average less than 30 dB HL and poor ear hearing threshold more than 70 dB HL (severe to profound hearing loss) were enrolled. Audiometric tests were administered in a sound treated two room setup with Grason-Stadler GSI-61 audiometer (Radioear Corporation, New Eagle, PA, USA) calibrated as per the ANSI S3.6 2010 standards. Patients of age <18 or >70 years, with history of a neurological insult or an ear infection in the last 3 months, intellectual disability, psychiatric or developmental disorders and diabetes were excluded. The patients were native speakers of Hindi as their primary language.
These patients underwent modified hearing in noise test (HINT) with different combinations of noise and speech signal. Three groups of reading were generated based on the poor ear status, whether it was 1) unaided, 2) aided with a Phonak wireless CROS B-312, i.e., behind the ear hearing aid and 3) aided with a cochlear BCD, i.e., cochlear BAHA 5 processor with Softband. Patients were assigned both the devices in a random order for one hour each and were tested in four different settings on the same day. Four different scenarios created for each group of readings as depicted in Fig. 1. Scenario Fig. 1A and B employed a noise source at the centre (0º azimuth) and speech signal presented once toward side of the poor ear (scenario Fig. 1A) and second towards the better ear (scenario Fig. 1B). This was followed by placing the speech signal at centre (0º azimuth) and presenting noise to the poor ear (scenario Fig. 1C) and to the better ear (scenario Fig. 1D) with the applicants sitting one meter away from the loudspeakers. The noise was presented at the fixed intensity level of 65 dB. Speech signal was decreased if the response was correct, and increased if the response was incorrect. The signal to noise ratio (SNR) at which subject is able to correctly identify the spondee words, 50% of the time was considered for the study. Lower SNR value indicates better speech perception and vice versa.
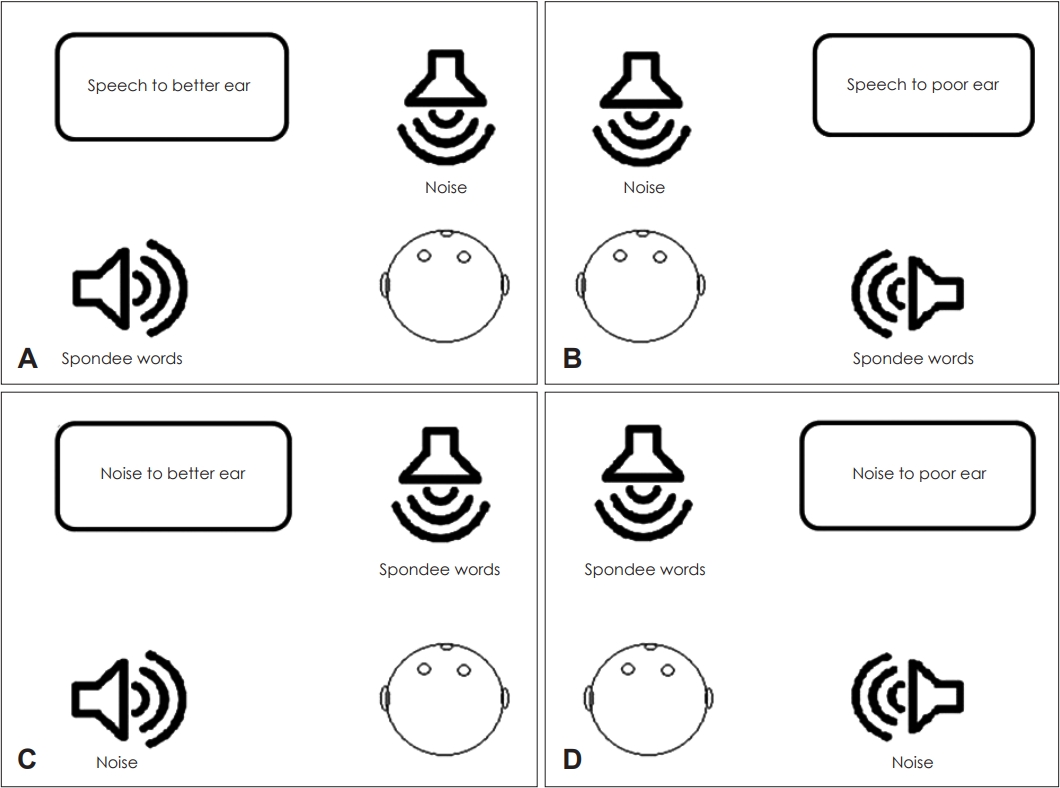
Modified hearing in noise test set up. (A) and (B) represent noise being presented to the patient from a loudspeaker at 0° azimuth and the speech at 90° azimuth from left and right ear respectively. (C) and (D) represent speech getting presented from 0° azimuth and the noise at 90° azimuth from left and right ear respectively.
SNR was compared among the unaided, BCD soft headband and CROS (in lateralized noise and lateralized speech in better and poor ear) using Friedman test whereas Wilcoxon signed-rank test with a Bonferroni correction was performed to evaluate statistical significance (p<0.05) difference between two different listening conditions since the data was not following normal distribution SPSS 21 (IBM Corp., Armonk, NY, USA) was used for analysis.
Results
Fifty-one patients with SSD participated in our study (43 males, 8 females) with a mean age of 23.2±6.8 years. The average duration of hearing loss was 9.04±10.8 years. Average pure tone bone conduction threshold in the better ear over 500, 1,000, 2,000, and 4,000 Hz was 17.04±5.10 dB HL with an average air- bone gap of 5.53±2.37 dB HL.
The ability to recognize speech was determined through the SNR scores. Fig. 2 represents mean SNR scores and significance for the unaided situation, with CROS and BCD in all the four scenarios of noise and signal presentation. The information obtained from the unaided state was considered as a baseline to compare the efficacy of the hearing devices.

Modified hearing in noise test set up. (A) and (B) represent noise being presented to the patient from a loudspeaker at 0° azimuth and the speech at 90° azimuth from left and right ear respectively. (C) and (D) represent speech getting presented from 0° azimuth and the noise at 90° azimuth from left and right ear respectively. *Significant difference present. SNR, signal-to-noise ratio; BCD, bone conduction devices; CROS, contralateral routing of signal; NS, not significant.
Noise at center and speech to the better ear (Fig. 2A)
SNR with the affected ear unaided was -1.47. In aided condition, SNR value was better with BCD (-3.82) and poorer with conventional CROS (-1.56). The BCD yields significantly better hearing than an unaided ear or the CROS hearing aid. There is statistically significant benefit from BCD but no audiological benefit of using a CROS hearing aid. This was the only scenario where one rehabilitation device (BCD) proved its superiority over the other (CROS).
Noise at the centre and speech to the poor ear (Fig. 2B)
SNR improved with the usage of any of the BCD (-1.27) or CROS (-1.86). The SNR was poorer with BCD in this scenario than CROS albeit statistically insignificant (p=0.365).
Speech at the center and noise at the better ear (Fig. 2C)
The CROS and BCD resulted in improved SNR (-1.18 and -1.67 respectively). Both devices (CROS and BCD) however did not yield any statistically significant benefit as compared to the unaided ear (p=0.333 and p=0.149 respectively). This was the only scenario where no statistically significant benefit was obtained from using either of the devices.
Speech at the center and noise at the poor ear (Fig. 2D)
SNR in the unaided, BCD and CROS was -0.88, -3.14, and -1.84 respectively. Both the devices yielded audiological benefit over the unaided ear (p<0.05) and also proved comparable. There was no significance advantage of a device over the other.
Discussion
Loss of binaural hearing leads to significant social handicap. The corporal effect instigated by diffraction of the signal by the head (head shadow effect) and speech discrimination in noisy surroundings (squelch effect) gets diminished. This study is an attempt to objectively measure the audiological benefit achieved by rehabilitative devices, i.e., BCD and CROS hearing aid. SNR calculated during a HINT is a standard way to measure this audiological benefit. Except the scenario where speech was presented at the centre and noise was presented to the better ear both aids indicated audiological benefit (though statistically significant only in 1st scenario). This signifies effective amplification with the aids which further will diminish the hitches enforced by sensory deprivation.
In 1st scenario (Fig. 2A), with noise in centre and signal presented to the better ear, BCD proved to be a better method of rehabilitation. This may be due to the fact that CROS aids cause occlusion effect in the better ear. A similar study by Hol, et al. [6-8] demonstrated better results with BCD. In the Hol, et al. [6] study, it was demonstrated that unaided ear yielded better SNR than an aided ear with a rehabilitative device (completely in the canal) when speech was lateralized to the better ear with centralized noise. This was perhaps due to better noise conduction from the centre by the aided ear. However, Markides [9] reported better SNR with CROS when signal was presented to the poor ear as in such situations CROS aid amplifies the noise and fodders it to the better ear. Kitterick, et al. [10], in their meta-analysis on the role of restoration and rerouting devices in SSD showed that a low SNR at the impaired ear leads to a hindered performance with rerouting. The meta-analysis recommended that patients may, therefore, require counselling to form an appropriate idea about when the rerouting device would prove useful and when it might be counterproductive. Lin, et al. [11] established that the ability to perceive speech in noise is superior with BCD as compared to an unaided ear and CROS. Similar results were shown in a literature review by Baguley, et al. [12]. This advantage of the BCD devices over the CROS aids is because of direct stimulation of the cochlea on the impaired side. Peters, et al. [4], however, demonstrated no advantageous effect of BCD or CROS in recognition of speech in noise. This postulates that both devices effectually widen the sound field through CROS by elevating head shadow effect. Whereas, Fogels, et al. [13] suggested better effect of CROS as compared to BCD which may be due to the fact that gain is insufficient in BCDs owing to using of softband.
When lateralized noise is presented to the better ear, both the hearing devices, CROS and BCD resulted in no benefit when compared to unaided ear which indicates the primary role of better ear in hearing even when the diseased ear is rehabilitated. Literature reports better SNR with CROS [14] and BCD [15,16] when noise is lateralized to better ear. This advantage is possibly due to the interference of noise with the speech signal when gets transmitted from the poor to the better ear. Unaided ears had lower SNR than aided ears (unaided, CROS, BCD: -7.1, -3.4, -5.5) when noise was presented to the poor ear [17]. This advocates that SSD individuals have learnt strategies for better perception from side of better ear. Similar results were reported by Mondelli, et al. [18] with rehabilitative devices. Contrary to this, there have been studies where both devices seem comparable in speech in noise performance [19-21].
The present study divulges the audiological benefits of rehabilitative devices in presence of noise in four different scenarios in Indian scenario in Hindi speaking adult SSD individuals with modified HINT test by making use of open ended Hindi phonetically balanced word list which makes the task complex for patients as compared to conventionally used closed ended sentences [7,13,21,22]. Moreover, contrary to other studies [7,17,23,24], participants were allocated the devices in a random order and performance of both the rehabilitative devices was examined on the same study and direct comparison amongst the devices was made in the unchanged sample of patients. Although, the verdict of a patient to use the aid is not just audiological in closed room situation, nonetheless outspreads the limits of objective outcomes in real life situations. Literature [25] reveals that the degree of accomplishment rests on the enthusiasm and the listening demands levied by the functioning environment of the patient. Further, no association was found between audiological benefits of rehabilitative devices and duration or etiology of SSD. Also, the study had no trial period for participants to adjust to the hearing devices. The current study does not measure these demands, nevertheless opens the avenue for more studies in real life situations.
In conclusion, SSD causes perception difficulty in certain social situations, like noisy surroundings. Though not a replacement for binaural hearing, auditory rehabilitation should be offered (CROS aid or BCD) as these devices enhance speech perception in noise. In most listening situations as tested by HINT scores, BCDs perform better than CROS hearing aids. Though they substantially overcome the head shadow and speech in noise upshot, they fall short when presentation of noise to the better ear suppresses its speech discrimination ability.
Acknowledgements
None
Notes
Conflicts of interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Kapil Sikka. Data curation: Rijendra Yogal. Formal analysis: Rijendra Yogal. Investigation: Mao Bhartiya. Methodology: Hitesh Verma. Project administration: Alok Thakar. Resources: Tanvi Chaudhary. Software: Rijendra Yogal. Supervision: Kapil Sikka. Validation: Chirom Amit Singh. Visualization: Sonam Sharma. Writing—original draft: Tanvi Chaudhary. Writing—review & editing: Rakesh Kumar. Approval of final manuscript: all authors.