Does Listening to Tinnitus Frequency-Filtered Music Relieve Tinnitus?
Article information

Abstract
Background and Objectives
Tinnitus frequency-filtered music therapy aims to restore lateral inhibition to reverse tonotopic reorganization in the auditory cortex. Although the tinnitus-relieving effect of this therapy has been investigated, the results remain controversial. We performed a prospective, randomized, controlled double-blind study to determine the tinnitus-suppressing effect of tinnitus frequency-filtered music therapy.
Subjects and Methods
The study included 90 participants who were randomly categorized into an experimental group that listened to tinnitus frequency-filtered music and a control group that listened to music from which a random frequency was removed. The Tinnitus Handicap Inventory (THI) score and measures of tinnitus loudness, daily awareness, and tinnitus-induced annoyance were evaluated at the initial visit and at 3 and 6 months (final follow-up). The rates of improvement in THI scores in the two groups were also recorded.
Results
All measured variables showed significant improvement in both groups, except the matched tinnitus loudness and minimal masking level. However, no significant intergroup differences were observed in the amount of improvement in THI scores and any other variable. The rates of improvement in THI scores were higher in the control group at 3 and 6 months.
Conclusions
Listening to tinnitus frequency-filtered music reduced tinnitus-induced handicaps; however, this approach was not significantly better than listening to music from which a random frequency was removed.
Introduction
Tinnitus is a common disorder with prevalence rates of approximately 10% in the general population and 30% in the elderly population. It can have a number of serious negative effects, including psycho-emotional symptoms such as distraction, insomnia, and depression. Therefore, chronic and persistent tinnitus often requires active intervention. However, there is no established treatment for this intractable disease.
Recently, Okamoto, et al. [1] developed ‘tailor-made notched music training (TMNMT)’ and suggested that it could reverse the tinnitus-generating mechanism, “maladaptive plastic changes (tonotopic reorganization) in the auditory cortex” by restoring lateral inhibition. TMNMT involves listening to music with an octave band centred on the patient’s tinnitus frequency filtered out (notched), to augment lateral inhibition of the notched region. Theoretically, this could enhance lateral inhibition by stimulating the lateral frequency regions rather than the overrepresented tinnitus frequency region [2,3]. The tonotopic reorganization model suggests that peripheral hearing loss reducing output from the damaged cochlear region may cause deterioration of lateral inhibition in the affected frequency areas and could subsequently enhance neural synchrony and hyperexcitability of the central auditory system, thus leading to develop tinnitus [4,5]. Pantev and colleagues [2,3] reported that TMNMT induced a reduction of auditory-evoked cortical activity corresponding to the tinnitus frequency, reflecting recovery of lateral inhibition. They also demonstrated behavioural and neural effects of TMNMT that did not depend on the filtered notch width (from 1/4 to 1 octave) or duration of treatment (where efficacy was seen even after only 5 days of treatment) [2,6]. However, only three randomized controlled studies regarding the tinnitus-relieving effect of TMNMT have been reported to date (two of which were reported by the developer’s group) and the results are controversial [7].
This prospective, randomized, controlled double-blind study was performed to comprehensively examine the tinnitus-suppressing effect of TMNMT. Patients in the experimental group listened to tinnitus frequency-filtered (tailor-made notched) music, while patients in the control group were provided with music stripped of a random frequency unrelated to tinnitus pitch.
Subjects and Methods
Study design
We performed a prospective, double-blind, randomized, controlled clinical study, in which 90 participants were randomly divided into two groups: the experimental group listened to music stripped of an octave band centred on the frequency corresponding to the individual’s tinnitus pitch, while the control group listened to music stripped of a random frequency unrelated to the tinnitus pitch. The participants provided audio files of their favourite music, which we modified according to the group allocation and then uploaded to their smartphones. The participants were instructed to listen to the modified music files for 2 h daily for 6 months. Hearing function and tinnitus were assessed at enrolment, and after 3 and 6 months. Institutional Review Board of Kangwon National University Hospital reviewed and approved the study protocol (IRB file number: KNUH-2015-11-001-032). The written informed consent was provided by all participants and we performed the study in accordance with Helsinki Declaration.
Participants
Participants were recruited in our hospital via posters, and from among tinnitus patients in our clinic from March 2016 to December 2020. The inclusion criteria were as follows: aged between 18 and 60 years, proficiency in using a smartphone, pure-tone average (PTA) threshold between 0 and 70 dB for frequencies of 250 Hz to 8 kHz, chronic pure tone or narrow band tinnitus (duration ≥3 months), unilateral or bilateral tinnitus with the same pitch in both ears, visual analogue scale (VAS) of daily tinnitus awareness ≥50% and a Tinnitus Handicap Inventory (THI) score ≥18. The exclusion criteria were vascular or somatic tinnitus or tinnitus that could be cured by known therapies; hyperacusis or auditory hypersensitivity unsuitable for music therapy; history of taking antidepressants or other psychotropic medications that could affect tinnitus; and inability to cooperate with the research. Subjects were excluded if they received other treatments for tinnitus, including drugs, during the follow-up period, or if they withdrew consent to participate in the study.
Hearing and tinnitus assessment procedures
Hearing assessment was performed in a double-walled soundproof room. Pure tone air (250 Hz to 8 kHz) audiometry, tinnitus frequency, loudness and minimal masking level (MML) matching were performed. Assessments of the tinnitus characteristics were performed, i.e., the THI and VAS of subjective tinnitus loudness, daily awareness and annoyance of tinnitus.
The tinnitus pitch was decided in two-alternative forced choice procedure: two frequencies of pure tones (or narrow band sounds) were presented for patients to choose the most similar sound to their tinnitus. In the order of 500 Hz/4 kHz pair, then 250 Hz/500 Hz pair or 4 kHz/8 kHz pair and so on, patients repeated the forced selection procedure in half-octave steps. The above procedure was repeated three times until the final frequency was decided.
Outcome measures
We defined THI score as the principal outcome measure because the total THI score could more comprehensively represent tinnitus-related functional, emotional and everyday life handicaps than other variables such as loudness or awareness of tinnitus. As additional measures, matched tinnitus loudness, MML and VAS scores of subjective tinnitus loudness, daily awareness and annoyance were assessed. All variables were measured at the initial visit, and at 3 and 6 months (final follow-up). In addition, we calculated the incidences of improvement in THI score ≥50% and ≥20% in the experimental and control groups at 3 and 6 months.
Data analysis
The SPSS program (v. 22.0; IBM Corp., Armonk, NY, USA) was used for statistical analyses. The patients’ initial demographic, hearing and tinnitus data and amount of improvement at 3 and 6 months (calculated as the difference between the initial and final values) in each variable were compared. Mann–Whitney U-test and chi-square test were applied for continuous and nominal variables, respectively. The amounts of improvement at 3 and 6 months were compared between the two groups using the paired t-test. p<0.05 was accepted as the statistical significance in all analyses.
Results
Ninety volunteers were initially enrolled in the study, with 41 and 33 continuing for 3 months, and 14 and 15 continuing for 6 months, in the experimental and control groups, respectively. We observed no significant difference in any initial demographic, hearing or tinnitus characteristic between the two groups (p>0.05) (Table 1). The total THI score improved significantly at 3 and 6 months in both groups. All VAS scores improved at 6 months in the experimental group, and at both 3 and 6 months in the control group. However, matched loudness and MML showed no improvement in either group (Fig. 1).

Initial demographic and audiologic profile of experimental and control groups
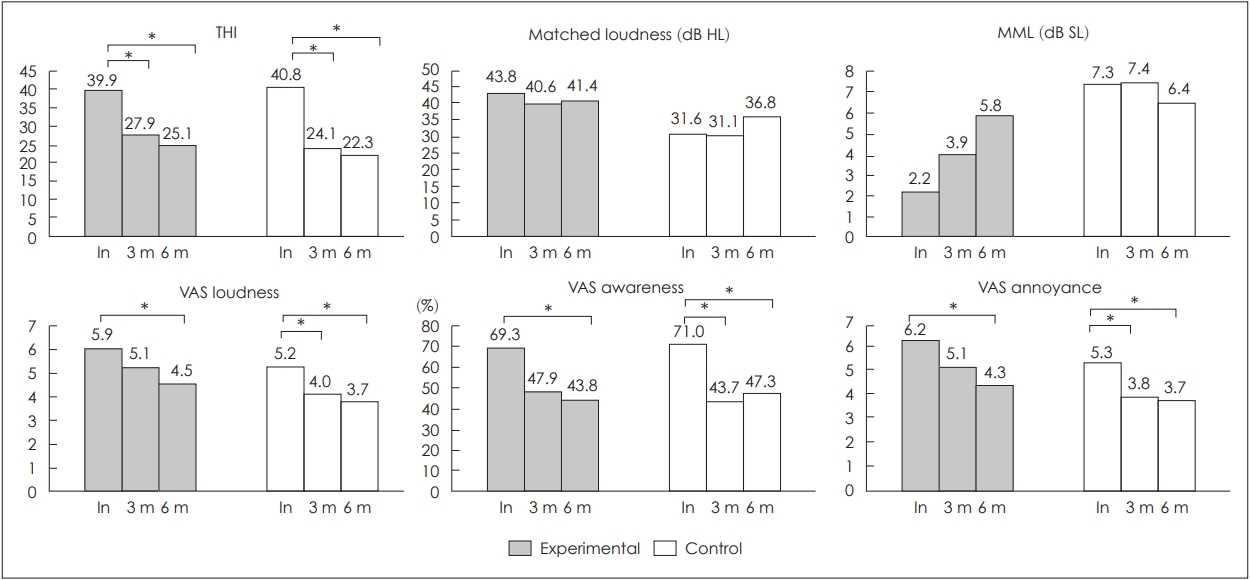
Tinnitus-related variables after 3 and 6 months of TMNMT (n=41 and 33 at 3 months, n=14 and 15 at 6 months in the experimental and control groups, respectively). THI and all VAS scores had improved significantly at 6 months in both groups, whereas matched loudness and MML showed no changes in either group (paired t-test, *p<0.05). In, initial; MML, minimal masking level; THI, Tinnitus Handicap Inventory; TMNMT, tailor-made notched music training; VAS, visual analogue scale.
There were no differences in the amounts of improvement in any variables between the two groups including THI scores: 12.0±13.4 vs. 16.7±15.1 and 14.8±12.4 vs. 18.5±14.5 at 3 and 6 months, respectively (Tables 2 and 3). The incidences of improvement in THI score ≥20% were 78.0% and 78.8% in the experimental and the control groups, respectively, at 3 months and 69.2% and 86.7%, respectively, at 6 months. The incidences of improvement in THI score ≥50% were 31.7% and 51.5%, respectively, at 3 months and 30.8% and 46.7%, respectively, at 6 months (Fig. 2).

Amount of improvement in tinnitus-related variables after 3 months of treatment

Amount of improvement in tinnitus-related variables after 6 months of treatment

Incidences of ≥20% (A) and ≥50% (B) reductions in THI score at 3 and 6 months of TMNMT (n=41 and 33 at 3 months, n=14 and 15 at 6 months in the experimental and control groups, respectively). The incidence rates of THI improvement were higher in the control group at both 3 and 6 months. THI, Tinnitus Handicap Inventory; TMNMT, tailor-made notched music training.
Discussion
The developers of TMNMT, Okamoto and Pantev, reported that it could reduce the awareness and loudness of tinnitus, and thus help alleviate the suffering of patients. In addition, they reported normalisation of tinnitus-related auditory cortical evoked activity (N1m component of the auditory steady-state response [ASSR]) on magnetoencephalography after listening to notched music, even for only 5 days [2,6,8-10]. However, we do not agree that the sound-evoked N1m response is an adequate marker for tinnitus-related activity, because tinnitus develops in the resting state without any external auditory stimulation. Rather, an abnormally elevated auditory-evoked response reflects hyperacusis, which frequently shows elevated gain in the auditory system. They also suggested that TMNMT could reverse the tonotopic reorganization seen in the auditory cortices of tinnitus patients, where tinnitus frequency is overrepresented in comparison to other frequencies because of increased spontaneous activity of the corresponding neurons [2,3]. However, tonotopic reorganization following auditory input deficit occurs only when hearing loss is severe, which has not been clearly demonstrated in tinnitus patients [11]. Furthermore, the recovery of tonotopic reorganization does not explain the effect of TNMNT, because sufficient hearing function is required to listen to the notched music, so patients with tinnitus associated with severe or profound hearing loss (a prerequisite for tonotopic reorganization) would not be good candidates for TNMNT.
Table 4 presents a summary of randomized, controlled double-blind studies on the tinnitus-relieving effect of TMNMT, including the present study. Taken together, there is no strong evidence to support the effectiveness of TMNMT, except in the reports by the developer’s group. They reported a greater improvement of VAS loudness by TMNMT compared to the control in one study with only eight participants, but showed no difference in a subsequent study, although there were positive effects on other variables such as a tinnitus questionnaire score and VAS awareness [3,12]. The study by Atipas, et al. [7] and our study assessed the effects of TMNMT more comprehensively and showed negative results for all measured variables; in particular, the indices of tinnitus loudness (matched tinnitus loudness, MML, or VAS score) were not significantly improved by TMNMT compared to the controls. There are clear discrepancies in results between Pantev’s group and other groups.

Randomized controlled double-blind studies on the tinnitus-relieving effect of treatment
In this study, we assessed changes in tinnitus at 3 and 6 months and observed no differences between the TMNMT and control groups at either time point. In addition, the incidence of THI improvement was higher in the control group at both 3 and 6 months (Fig. 2). It is noteworthy that the control treatment (listening to randomly filtered music) significantly alleviated suffering from tinnitus, which suggests that listening to music (regardless of filtering) could relieve tinnitus possibly via distraction, acoustic masking or psychological relaxation.
A Cochrane meta-analysis reviewed 590 studies on tinnitus-relieving effect of sound therapy (using hearing aids and/or sound generators) and concluded, “There is no evidence to support the superiority of sound therapy for tinnitus over waiting list control, placebo or education/information with no device [13].” It could support the negative results of this study and the power of the placebo effect.
In the study by Atipas, et al. [7] about 60% of the initially enrolled patients completed the 6-month treatment, while we had a completion rate of only 32%; this may represent a major limitation of the present study.
In conclusion, the mechanism of tinnitus-frequency filtered music therapy (TMNMT) is unproven (recovery of tonotopic reorganization), and the developers’ studies used an inadequate neurological marker for tinnitus activity (N1m component of ASSR). Moreover, the results were inconsistent even in their own studies, and there is no reliable evidence of the effectiveness of TMNMT for the treatment of tinnitus. Music therapy, a unique form of sound therapy, appears to have a potential to relieve tinnitus; however, higher-quality research is needed to develop a more effective methodology that addresses optimized stimulation parameters and duration of treatment, and the best responding tinnitus populations.
Acknowledgements
None
Notes
Conflicts of interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Shinyoung Yoo, Eui-Cheol Nam. Data curation: Shinyoung Yoo, Natalia Yakunina. Formal analysis: Natalia Yakunina. Investigation: all authors. Methodology: all authors. Project administration: Shinyoung Yoo, Eui-Cheol Nam. Resources: Shinyoung Yoo, Eui-Cheol Nam. Software: Natalia Yakunina, Eui-Cheol Nam. Supervision: Eui-Cheol Nam. Visualization: Natalia Yakunina, EuiCheol Nam. Writing—original draft: Shinyoung Yoo, Eui-Cheol Nam. Writing—review & editing: all authors. Approval of final manuscript: all authors