Introduction
Being equipped with an appropriate hearing instrument is the first step for children with hearing loss (HL) to learn to communicate through listening and speaking. Both validation and verification are required for hearing aid fittings to ensure the settings are optimized and the user receives sufficient and adequate auditory access. Validation is a subjective measure usually completed through a questionnaire of user satisfaction with amplification so that the requirements for everyday communication can be met. However, because the existing self-report questionnaires of hearing aid satisfaction were mainly designed for school-age children (e.g., Children’s Home Inventory for Listening Difficulties, Listening Situations Questionnaire) [1,2], the hearing aids validation for younger children often has to rely on parental observation. Although parental reports allow audiologists to gain insight into children’s responses to sound, the reliability of the feedback can depend on whether parents can distinguish between responses induced by auditory events and those induced by a combination of auditory and visual features. To overcome this limitation, quick speech sound tests such as the Ling Six Sound Test [3] and the Chinese Sound Test [4] are often recommended to parents because their testing procedures are straightforward, and parents can use these tests to monitor the status of a child’s hearing at different frequencies. In addition, these tests provide frequency-specific results according to which audiologists can adjust hearing aids.
Verification is an objective measure and commonly involves a coupler-based test box and a real-ear measurement (REM) system [5]. Electroacoustic assessments using a test box ensure that the performance of hearing aids meets their original specifications [6]. REM is an aspect of the recommended practice for hearing aid verification and can determine whether the gain and output of the hearing aid match the targets prescribed for the user [7-9]. However, despite the professional guidelines, electroacoustic measurement and REM are not routinely performed. The hearing aid test boxes required for electroacoustic analysis (e.g., AudioScan Verifit and RM500) are not always available in every clinical center for various reasons (e.g., lack of time or financial difficulties) [10]. In addition, real-ear verification can be impractical and unfeasible for infants and young children because it requires time and cooperation [11].
Despite being controversial, aided sound field testing, also known as “functional gain testing”, is a viable alternative to examine aided performance [12-14]. However, obtaining reliable behavioral audiograms in pediatric practice can be particularly challenging because of children’s short attention span and immature cognitive development. Test stimuli with broader bandwidths should be used to maintain children’s interest in a signal [15]. Narrow-band noise (NBN) and warble tones are two common alternatives to pure tones that are used when performing sound field testing. However, in pediatric practice, obtaining responses by testing with warble tones can be difficult, and testing with NBN may overestimate or underestimate performance, especially for sloping or rising audiograms [13,16]. Thus, audiologists must be able to determine whether the results of a child’s aided hearing performance test are plausible and whether they fall within the same range as those of other children with similar degrees of HL.
Speech stimuli such as frequency-specific sounds (e.g., Ling’s six sounds) are often used to validate aided auditory function in pediatric practice. Compared with NBN, speech stimuli can more easily elicit a child’s attention, and the response level for this method for children aged 2 years or younger is approximately 25 dB HL lower than that for NBN [17]. When no audiogram is available, the awareness threshold for frequency-specific sounds can be used for cross-checking and function as an initial guidance of hearing aid fitting. Frequency-specific speech sounds are not only useful for the daily monitoring of hearing but can also be used in routine hearing evaluations to cross-check the responses on an audiogram, especially when NBN or warble tone results are not reliable.
Scollie, et al. [18] confirmed the benefits of using Ling’s six sounds to measure aided speech detection thresholds and developed the Ling-6(HL) test, an assessment tool designed for use in clinical settings. Based on their assessment, other researchers [19] developed the pediatric Ling-6(HL) scoring sheet, which indicates the typical performance range for children with typical hearing (TH) and the typical aided performance range for children with mild, moderate, or severe HL.
However, the Ling-6(HL) scoring sheet is based on American English and therefore may only be reliable for native English native speakers. Some research has indicated that materials in native and nonnative languages can yield different behavioral and electrophysiological responses [20]. Clinicians should therefore consider linguistic differences to increase diagnostic accuracy and ensure clinical reliability. Some researchers have attempted to adapt language-based assessments to a target language. For example, the six Mandarin sounds /u, ə, a, i, tɕʰ, s/ were selected for the Chinese Sound Test because of their high level of frequency specificity, early age of acquisition, and low articulatory variability [21]. As with the Ling six sounds, the Chinese Sound Test was examined for its reliability, but instead of clinical settings, it was examined for use in daily life. The results confirmed that the Chinese Sound Test can reflect hearing thresholds, indicating its crucial role in monitoring fluctuating hearing [22].
To the best of our knowledge, the exact relationship between Mandarin speech sounds and NBN in aided sound field testing remains unclear. Although several studies have investigated this topic, they have all focused on Ling’s six sounds [23]. To provide audiologists with a reliable tool with which to verify the performance of hearing aids for Mandarin-speaking children, this study developed the Mandarin Phoneme Detection Score Sheet based on the ideas of Glista, et al. [19] and Scollie, et al. [18] and examined the relationship between detection thresholds of speech sounds and audiometric hearing thresholds across frequencies.
Subjects and Methods
Participants
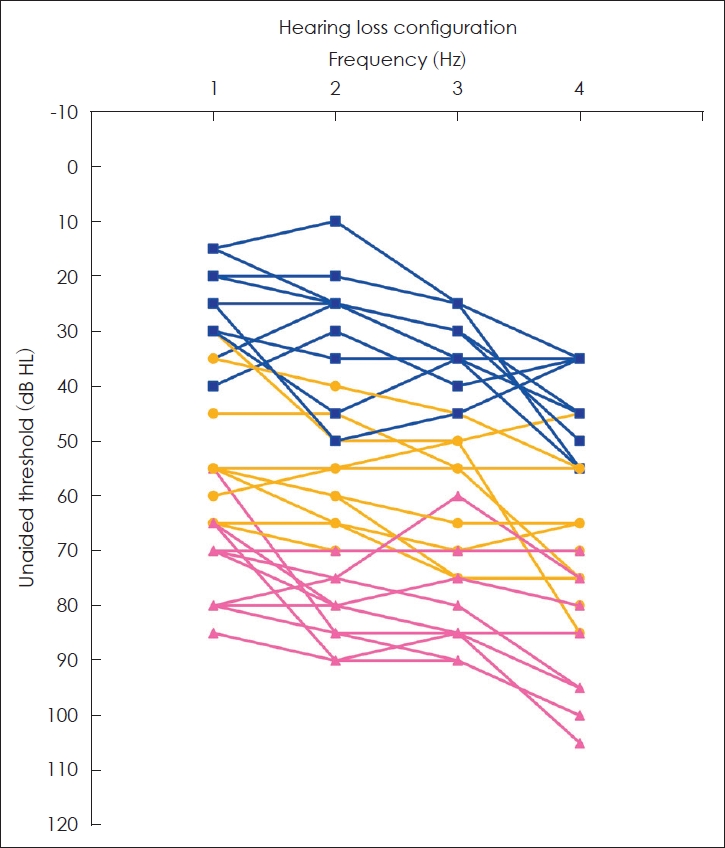
To establish the typical detection threshold of each speech sound, 30 adults with TH (age range: 20-35 years; mean age: 27.1 years; standard deviation [SD]: 3.9) were recruited. Their mean hearing thresholds (500-4,000 Hz) ranged from -10 to 15 dB HL (mean=6 dB HL, SD=6). Of the 30 participants, 20 participated in the transformation test (age range=20-34 years; mean age=28.05 years; SD=3.8). The transformation test was conducted to obtain the calibration value of each Mandarin phoneme. As shown in Table 1, the calibration value was used to normalize the detection threshold to 0 dB HL for the subsequent formal test. Their mean hearing thresholds (500-4,000 Hz) ranged from -10 to 15 dB HL (mean=7 dB HL, SD=6.2). Of the 30 participants, 10 participated in the formal test (age range=20-30 years; mean age=25.10 years; SD=3.5). Depending on the phoneme presented in the formal test, the corresponding calibration value was added to the threshold value (i.e., the dial value) to yield the normalized final test result. Their mean hearing thresholds (500-4,000 Hz) ranged from -5 to 15 dB HL (mean=4 dB HL, SD=4.7) (Table 2). To establish the corresponding range of aided detection thresholds for each hearing degree, we then recruited 30 children with HL (age range=3-12 years; mean=6.7 years; SD=2.4). As shown in Supplementary Table 1 (in the online-only Data Supplement), the cohort was divided into three subgroups on the basis of the degree of HL: mild HL (mean=33 dB HL, SD=4.8, n=10), moderate to moderately severe HL (mean=59 dB HL, SD=8.9, n=10), and severe HL (mean=78 dB HL, SD=6.6, n=10) (Fig. 1). All children with bilateral HL wore hearing aids during testing, the hearing aid information is presented in Supplementary Table 2 (in the online-only Data Supplement). All hearing aids were verified using Desired Sensation Level (DSL) version 5.0 target gain [24]. Age-appropriate real-ear-to-coupler differences were used to verify the hearing aid settings. An output gain of 250-4,000 Hz was measured to ensure that at least four out of five frequencies matched the DSL version 5.0 target gain (tolerance value: sound pressure level [SPL] of ±5 dB) (Supplementary Table 2 in the online-only Data Supplement). The otoscopy and tympanograms were examined for all the participants before testing.
Materials
Six Mandarin phonemes (/u, ɤ, a, i, tɕʰ, s/) identified as clinically important to aural rehabilitation in Hung and colleagues [21,22] were selected. These phonemes were selected for their frequency specificity, early age of acquisition, and intraarticulatory and inter-articulatory stability. Another seven Mandarin phonemes with varying manners of articulation were selected as distractors. Nasal stop /m/, stops /p, t, kh/, affricates /tʂ/, and fricatives /ɕ, f/ were added to the test to ensure that the participants were unaware of the purpose of the experiment. Mandarin phonemes that speakers could not correctly or properly pronounce, such as retroflex /tʂ/ produced as deretroflex /ts/, and those that speakers produced too strongly were excluded because they could not be analyzed on the spectrogram. A female native Mandarin speaker (aged 30 years) without speech, language, or voice problems produced the speech stimuli for the test. Each speech sound was produced three times with a fundamental frequency ranging between 245 Hz and 250 Hz (mean=248.49 Hz). Each consonant is pronounced alone without adding vowels after it to avoid the transition acoustic cues between the consonant and vowel. An AKG acoustic microphone (AKG, Northridge, CA, USA) was used for recording, and the distance between the speaker’s mouth and the microphone was 30 cm. The microphone specifications are as follows: 20-20,000 Hz audio frequency bandwidth, cardioid polar pattern, 20 mV/Pa sensitivity, 16 dBA equivalent noise level. Speech materials were recorded in a soundproof booth by using Praat (version 5.3.85; https://www.praat.org/) at a sampling rate of 44,100 Hz quantized at 16-bits. A total of 39 waveform files were created, and vowels were selected if they were stable and had a length of approximately 1 s. Consonants were selected if the peak of their waveforms did not exceed the analysis window. The first sound item was always selected when multiple vowels/consonants met the criteria, as the speaker usually produced the first sounds with more strength. Because it is difficult to prolong the length of stops and affricates during pronunciation, the speaker was asked to pronounce each sound naturally, and do not change the articulation to achieve certain duration. The researchers maintained the original sound files and did not lengthen the sounds using the software but repeated them three times to achieve the same temporal length as the vowels. The original duration of each consonant was about 300-310 ms, and that of vowel was around 950-960 ms. To maintain the acoustic characteristics and the similar duration of each sound file, the duration of consonant was normalized into 290 ms, and that of vowel was 940 ms. The files had 30 ms of silence at the beginning and end. The intervals between the consonant stimuli were also 30 ms. After normalizing the duration and intensity of the 13 phonemes, each sound trial lasted 1,000 ms with a 70 dB-SPL. The acoustic information of F1 and F2 was measured by selecting the whole vowel and using the Formant function in Praat. The program then displayed the mean F1 and F2 of the selected vowel. For consonants, the spectral moments were measured. The consonant was selected, and the Spectrum function was used to view the spectral slice. After the spectral slice file was obtained, Query was used to obtain the center of gravity, which indicated the largest amount of energy centralized in a frequency range. Table 3 lists the acoustic information of the six target stimuli. Finally, four randomized presentation lists were generated to avoid potential order effects.
Procedures
This study was conducted by audiologists in a two-room sound suite (ANSI S3.1.1991; American National Standards Institute, New York, NY, USA). All audiometric threshold measurements were performed using a Grason–Stadler model 61 (GSI 61, Grason–Stadler, Eden Prairie, MN, USA) audiometer with loudspeakers (GSI high-performance speakers) located 1 m to the left and right of the seated participant at a 45° azimuth approximately 1 m above the floor. NBN was used to assess the detection thresholds in the sound field when the participants were wearing bilateral hearing aids. The NBN sound field thresholds of the participants were obtained at 250-6,000 Hz. The NBN and Mandarin phoneme detection thresholds were assessed in the sound field in accordance with the Hughson–Westlake technique [25], which is a widely used pure tone test procedure (ANSI S3.21-2004). The participants were instructed to raise their hands when they detected a sound. When a child heard a sound, the intensity was decreased by 10 dB, and when the child did not respond to the sound, the intensity was increased by 5 dB. The threshold of NBN and phoneme detection was obtained when 50% correctness was achieved. The procedure lasts approximately 1 hour. After the threshold data were collected, the transformation test was performed. First, the thresholds of the 20 adults with TH for NBN (250-6,000 Hz) were obtained. The pure tone averages must be within 25 dB HL. Second, the thresholds of the 20 adults with TH for the 13 Mandarin phonemes were obtained, and the values were calibrated into dB HL. The calibrate values were used as a reference when the other 10 adults with TH and children with HL were tested in the formal test (Table 1).
Statistical analysis
SPSS version 23 (IBM Corp., Armonk, NY, USA) was used for the statistical analysis. The typical threshold range for detecting phonemes was established based on the results of the TH testing. The aided NBN and phenome detection threshold ranges for HL were estimated using 95% confidence intervals. First, the average threshold of each phoneme was obtained, and the 95% confidence interval was calculated. Then, the upper limit of the 95% confidence intervals was obtained, and the researchers corrected the value to 5-dB steps to match the audiogram. For example, if the average threshold of /m/ is 22 dB, the upper limit of its 95% confidence intervals is 27 dB, which is then corrected to a 5-dB step, and the final threshold of /m/ becomes 30 dB HL. A Pearson’s correlation test was performed to examine the relationship between the aided NBN thresholds and the phoneme detection thresholds. A stepwise regression analysis was performed to identify NBN frequency thresholds that were accurate predictors of phoneme detection performance.
Results
Mandarin phoneme detection thresholds
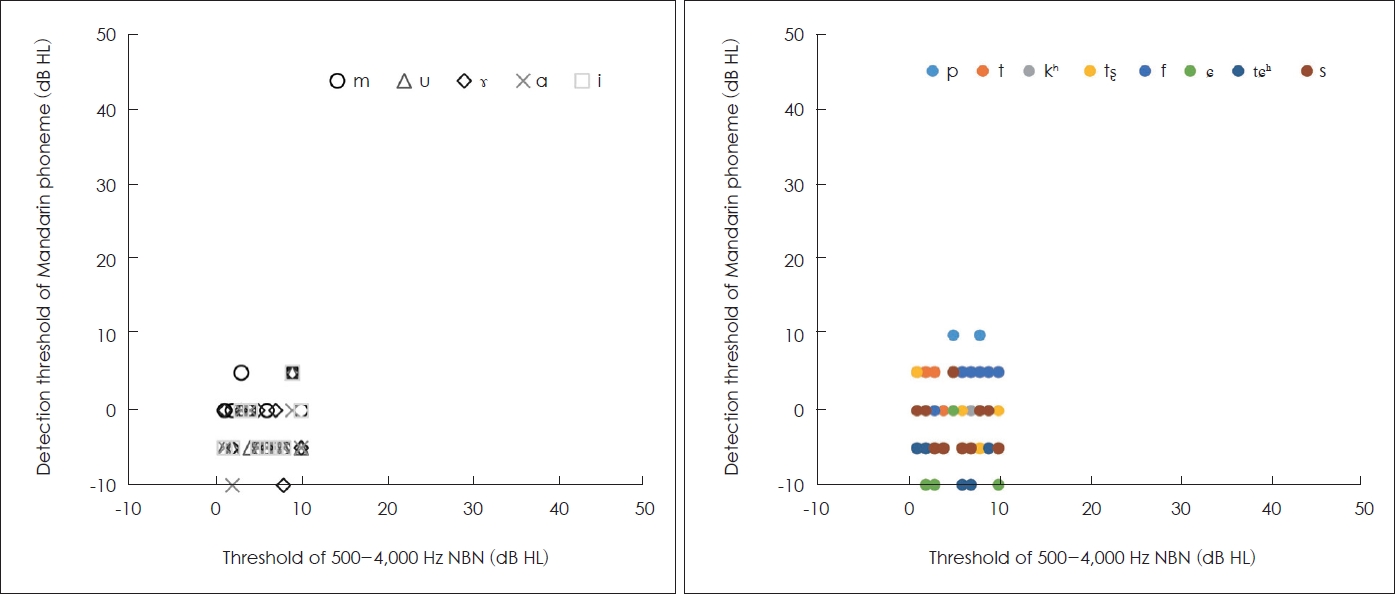
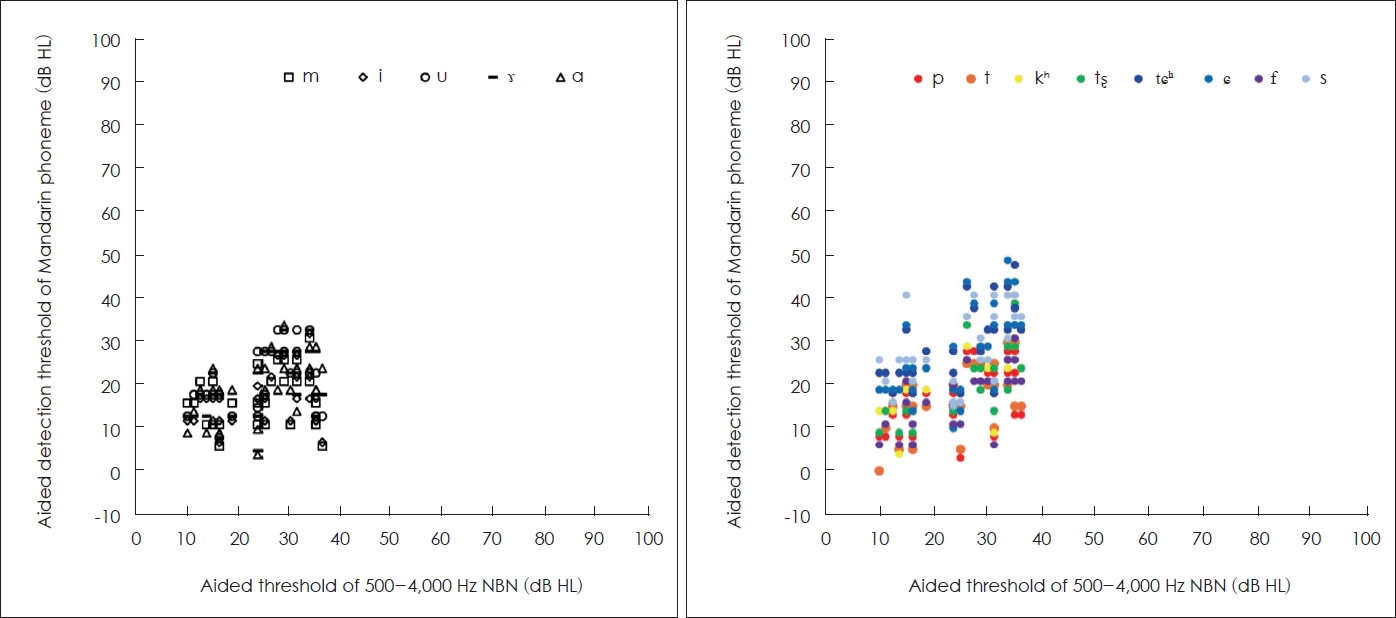
The Mandarin phoneme detection thresholds for TH were -10 to 10 dB HL (mean=-1.27 dB HL, SD=4.6). The detection thresholds for nasals and vowels were -10 to 5 dB HL (mean=-2.5 dB HL, SD=3.7), and those for consonants were -10 to 10 dB HL (mean=-1, SD=4.9) (Fig. 3). For children with mild HL, the detection thresholds for nasals and vowels were 4-27 dB HL (mean=13.90 dB HL, SD=4.62), and those for consonants were 1-28 dB HL (mean=15.92, SD=6.25). For children with moderate to moderately severe HL, the detection thresholds for nasals and vowels were 12-34 dB HL (mean=21 dB HL, SD=5.51), and those for consonants were 3-46 dB HL (mean=23.43, SD=8.22). For children with severe HL, the detection thresholds for nasals and vowels were 7-33 dB HL (mean=23.20 dB HL, SD=6.92), and those for consonants were 6–51 dB HL (mean=28.28, SD=9.78) (Fig. 4).
Correlations between aided NBN thresholds and Mandarin phoneme detection thresholds
The statistical analysis revealed that the aided NBN thresholds and the Mandarin phoneme detection thresholds were significantly correlated in most of the frequencies (Table 4). The strongest correlation for /u, ɤ/ was found at 500 Hz (/u/: r=0.53, p=0.003; /ɤ/: r=0.56, p=0.001). The strongest correlation for /a/ was found at 1,000 Hz (r=0.51, p=0.004). The strongest correlation for consonants /tɕʰ, s/ was found at 6,000 Hz (/tɕʰ/: r=0.76, p<0.001; /s/: r=0.64, p<0.001). For /i/, marginal significance was observed both at 500 Hz (r=0.35, p=0.061) and at 1,000 Hz (r=0.35, p=0.062).
Prediction of aided NBN thresholds based on Mandarin phoneme detection thresholds
The prediction of aided NBN thresholds based on Mandarin phoneme detection thresholds indicated that phoneme /ɤ/ can predict the aided thresholds of 250 Hz (r2=0.184, p=0.029) and 500 Hz (r2=0.269, p=0.007); /a/ can predict that of 1,000 Hz (r2=0.304, p=0.004), 2,000 Hz (r2=0.250, p=0.009), and 4,000 Hz (r2=0.245, p=0.010); and /tɕh / can predict that of 6,000 Hz (r2=0.657, p<0.001). No significant results were observed for /u, i/ or /s/ (Table 5).
Although the aided thresholds of NBN were significantly correlated to the Mandarin phoneme detection thresholds at most frequencies, the results of the stepwise regression analysis indicated that only thresholds at certain frequencies were good predictors of Mandarin phoneme detection performance and vice versa.
Mandarin Phoneme Detection Score Sheet
According to the results (Supplementary Tables 3-5 in the online-only Data Supplement), the Mandarin Phoneme Detection Score Sheet (Fig. 2) can offer clinicians a reliable reference with which to estimate NBN thresholds based on Mandarin phoneme detection performance. This can be especially helpful to pediatric audiologists for cases in which NBN results with no or limited reliability can be obtained. The upper limits for TH, mild HL, moderate to moderately severe HL, and severe HL indicate the highest threshold observed in each subgroup and are represented in Fig. 2 by the green line, blue line, yellow line, and red line, respectively. Audiologists can quickly determine the appropriateness of hearing aid fitting by referring to this index.
Discussion
The four auditory development stages are detection, discrimination, identification, and comprehension [26]. The ability to detect sounds is the foundation and a prerequisite for developing auditory skills. Therefore, this study selected a detection task for testing. However, the ability to detect sounds does not necessarily ensure the ability to discriminate sounds, as research has indicated [27]. Nevertheless, aided detection thresholds determine the minimum audible frequency range. Aided detection thresholds are significantly correlated with word recognition scores obtained at the soft level [28]. Speech recognition improves with aided thresholds, which results in the audibility of a greater proportion of speech signals. Measurements of aided sound field thresholds should not be used as the only method of hearing aid verification [29]. Although detection tasks alone are insufficient, they provide valuable information to clinicians with which to assess the audible range of children who are too young or developmentally delayed for standard speech recognition tests.
The Mandarin Phoneme Detection Score Sheet is the first Mandarin phoneme screening tool, which can be more suitable while screening Mandarin population. Furthermore, the present study is the first study to examine the relationship and predicted power of the thresholds between Mandarin phonemes and NBN. The results of the present study provide an evidence-based tool for clinical use.
Use of phoneme detection to predict aided sound field performance
Pediatric patients tend to respond better to speech stimuli than to pure tones or warble tones. Therefore, a speech sound detection test should be performed first during behavioral hearing testing to quickly measure a child’s detection ability [15]. Fig. 2 is presented to provide clinicians with a convenient screening tool to quickly cross-check aided performance. For example, detection of the /ɤ/ sound should ensure the detection of 250-Hz and 500-Hz NBN at least at the 20-dB HL level for children with mild sensorineural HL (SNHL). For children with severe SNHL, detection of the /tɕʰ/ sound should ensure the ability to perceive 6,000-Hz NBN at least at the 50-dB HL level.
This study demonstrated that Mandarin phoneme detection thresholds predict aided NBN detection thresholds; the phoneme /ɤ/ predicts the aided thresholds of 250 Hz and 500 Hz; /a/ predicts those of 1,000 Hz, 2,000 Hz, and 4,000 Hz; and /tɕh/ predicts that of 6,000 Hz. The results revealed that only /ɤ, a, tɕʰ/ can be used, which indicates that despite the significant correlation between phonemes and certain frequencies, acoustic cues do not directly reflect perception performance. The use of Mandarin phonemes to predict the aided detection threshold of NBN should be approached with caution during clinical procedures.
Clinical implications for hearing aid prescriptions in Mandarin
The Mandarin phoneme /s/ is of a higher frequency (7,000-8,998 Hz) than its English (6,000-8,000 Hz) counterpart [21]. In addition, some Mandarin phonemes do not exist in English, such as /tɕ, tɕʰ, ɕ, ts, tsʰ/. These phonemes also have high-frequency energy of approximately 6,000-7,000 Hz [30]. The phonemic differences between English and Mandarin demonstrate the potential need to prescribe more amplification for frequency ranges of 6,000 Hz or above to provide sufficient audibility for the detection of Mandarin consonants. The results of this study also revealed linguistic differences between English and Mandarin, elucidating the potential need for language-specific hearing aid prescriptions. No hearing aid prescription algorithm based on the linguistic and acoustic characteristics of Mandarin has been established for clinical use. Mandarin-speaking children with HL are typically prescribed hearing aids by using DSL version 5.0 [24].
The Ling-6(HL) scoring sheet developed by Glista and colleagues [19] and the Mandarin Phoneme Detection Score Sheet (Fig. 2) developed in this study both assess perceptual abilities only at the level of detection. Listeners’ responses in the aided range do not necessarily imply the recognition of particular sounds. Despite the similar aided ranges of the Ling-6(HL) test audiogram and the Mandarin Phoneme Detection Score Sheet, a hearing aid prescription algorithm derived from the acoustic characteristics of Mandarin must achieve optimal amplification for Mandarin listeners to increase speech recognition performance.
Limitations and future research
Although this study attempted to provide clinicians with a useful method of using Mandarin phonemes to cross-check the status of young children’s hearing, several limitations must be addressed. First, this study was limited by its small sample size, which may prevent its results from being generalized or applied to specific target groups. Additional studies with a larger number of participants are required to produce more reliable findings.
Second, this study developed the screening tool by using recorded materials. Therefore, the Mandarin Phoneme Detection Score Sheet should be used with the recorded sound files (Supplementary Audio 1-6 in the online-only Data Supplement) to obtain reliable results. Numerous factors can affect acoustic characteristics, such as the gender, age, and voice quality of a speaker [30]. Future research should consider these factors and explore their impact on phoneme detection.
Finally, to expand the use of this screening tool to various applications, unaided Mandarin phoneme detection performance data should be collected to establish an unaided version of the scoring sheet. Similarly, a systematic investigation of various auditory stimuli, such as warble tones and pediatric noise, should be conducted.
Conclusion
The Mandarin Phoneme Detection Score Sheet was developed by examining the ability of Mandarin phonemes to predict the NBN threshold and identifying a frequency-specific correlation between Mandarin phonemes and NBN thresholds. This tool can aid clinicians in determining whether aided performance falls within the expected range for younger children and in cross-checking the results of audiometric testing, especially during the first few hearing aid fitting sessions.