Introduction
Presbycusis, also known as age-related hearing loss, refers to age-related, sensorineural hearing impairment in elderly individuals [1,2]. Commonly, the term “elderly” refers to individuals of age ≥65 years, however, presbycusis may also present if one has a hereditary predisposition, chronic noise exposure, vascular disorder diabetes mellitus, etc. [3]. In the United States, approximately half of the people aged ≥65 years have some degree of hearing loss [4]. As the elderly population is increasing worldwide [5], it is natural that the number of patients with presbycusis is also increasing. In October 2021, the percentage of elderly individuals in Korea was 17.0% and it was predicted to increase [6]. Presbycusis can be overlooked because it is so prevalent; however, it is a critical condition that affects not only the physical, cognitive, and emotional activities of patients, but also their social functioning [7]. The common symptom of presbycusis is the progressive and symmetric loss of high-frequency hearing over several years. Additionally, it may also be accompanied by tinnitus, vertigo, and disequilibrium [8].
Furthermore, recent studies have shown that presbycusis is associated with several other problems, and one study found that resolving hearing loss could contribute to a reduction in the prevalence of cognitive impairments such as dementia. Even the mechanism of the potential link between hearing loss and cognitive impairment is constantly being raised [9].
The natural history of presbycusis shows that it is an irreversible disease that tends to worsen over time without medical help. As is known from several animal experiments, presbycusis does not recover over time, but rather increases the threshold for hearing [10]. The results of animal experiments conducted so far have shown that the way to recover the deteriorated hearing is unknown [11]. Therefore, considering these factors, the early prevention of presbycusis is the priority. The assistive options for presbycusis include a variety of rehabilitation techniques, hearing aids, cochlear implantation, and assistive pharmacological therapy. Additionally, various treatments such as stem cell therapy and gene therapy are being tried recently [12,13]. Notably, the application of these preventive therapies has limitation; therefore, it is necessary to develop new treatment methods.
Meanwhile, among the drugs that have been used to manage presbycusis and its associated symptoms, such as tinnitus, are Ginkgo biloba and choline alfoscerate. Ginkgo biloba, known to act as antioxidant and enhance cerebral and vestibular blood flow [14,15], has been widely used for tinnitus, which is one of the symptoms associated with presbycusis [16]. Animal studies showed that Ginkgo biloba increases auditory brainstem activity, which leads to an increased thalamic input to the primary auditory cortex, thereby alleviating tinnitus [17]. Clinical studies also showed that Ginkgo biloba is effective in alleviating tinnitus and dizziness in patients with dementia [18]. Additionally, choline alfoscerate, known to act on cholinergic hyperfunction, has been used to treat mild to moderate Alzheimer’s disease and used partly as an auxiliary treatment in patients with presbycusis [19,20]. It is closely related to presbycusis because recent studies have shown that neuropathy is associated with hearing loss and cognitive impairment. That is, the neuronal degeneration of hearing loss, inhibition of neurogenesis, increase in tau-protein, and neuroinflammation in the hippocampus are the links between presbycusis and cognitive impairment.
Ginkgo biloba is a drug that is often used alone to control tinnitus; however, its effect on hearing is insignificant [21,22]. Although choline alfoscerate has been reported to enrich listening comprehension in older age, it has still not been studied much at present, especially in areas such as pure tone audiometry (PTA) [23]. Additionally, the clinical effects of Ginkgo biloba are not yet elucidated. Therefore, in this study we attempted to analyze the differences between Ginkgo biloba monotherapy (hereinafter referred to as monotherapy) and Ginkgo biloba and choline alfoscerate combination therapy (hereinafter referred to as combination therapy). If the advantage of combination therapy is greater than that of monotherapy, it would be appropriate to use the combination therapy, otherwise, it would be an overdose of the drug. Furthermore, if monotherapy shows better results than the negative control groups, the combination therapy could be added as a necessary option for patients with senile hearing loss by syllogism. Therefore, we reviewed patients treated in our hospital retrospectively to ascertain whether there are advantages to using combination therapy, and to identify the advantages, if present.
Subjects and Methods
Study population
This retrospective study was performed using the medical profiles of patients, aged ≥65 years and diagnosed as having presbycusis and treated in the Department of Otorhinolaryngology, Wonju Severeance Christian Hospital. The study was approved by the Wonju Severeance Christian Hospital Institutional Review Board (IRB No. CR321135). We also collected the medical profiles of patients who did not take any medication for presbycusis and only used hearing aid for presbycusis, as the negative control group. The two drugs for presbycusis included: 1) ginkgo leaf dried extract 80 mg, 2 times a day, and 2) choline alfoscerate 400 mg, 2 times a day. The medical files used in this study were obtained from patients who visited the institution between January 2015 and May 2021. Additionally, the wash-out period was also set up as 6 months after the investigation period (June 2021 to November 2021) for the Kaplan–Meier curve, which is usually used to predict the survival period of data.
We excluded patients with the following conditions: 1) patients with a history of audiologic surgery; 2) patients who had or were suspected of having sudden hearing loss, noise-induced hearing loss, Bell’s palsy, vestibular neuritis, or other audiologic medical conditions before; 3) patients who were treated with other treatment methods that may affect the evaluation of this study, such as hyperbaric oxygen therapy, intratympanic steroid therapy, oral steroid medication; 4) patients who were not followed up regularly within the criteria for selecting a suitable period for the study; 5) patients who did not regularly take prescribed medications; and 6) the medical profiles of patients which were judged as unsuitable for the study by the clinical trial director.
Following these criteria, a total of 197 medical files (119 patients who used Ginkgo biloba only and 78 patients who used Ginkgo biloba and choline alfoscerate combination therapy) were selected for study inclusion.
The composition of the population-sample group, selected group, and excluded patients based on these criteria is shown in Table 1. The number of individuals corresponding to the final population was obtained by sequentially subtracting from criteria 1 to 6.
For the selection of the control group, the criteria of a person who had not received any treatment other than a hearing aid was included in the inclusion criteria above. With respect to the exclusion criteria, all criteria, except criterion 5, were applicable to the control group. As a result, 60 cases were grouped into the negative control group.
Treatment protocol
All the patients in the experimental group reviewed retrospectively were prescribed ginkgo leaf dried extract 80 mg alone or a combination of ginkgo leaf dried extract 80 mg and choline alfoscerate 400 mg. Subsequently, the patients visited the hospital at regular intervals and received regular follow-up using PTA.
In the control group, the hearing of non-medicated, patients managed with hearing aids was periodically followed up. On the first day of hospitalization, a routine laboratory test (complete blood count, chemistry), chest radiography, electrocardiogram, and other examinations were conducted to rule out other underlying diseases.
Interval of data collection
The data of patients who had been prescribed Ginkgo biloba or choline alfoscerate during the investigation period were collected from 3 to 6 months, 6 to 9 months, 9 to 12 months, and 12 to 15 months from the date of the first diagnosis.
However, the data of patients managed with hearing aids had to have longer investigation intervals because the normal follow-up period after wearing hearing aids was not as short as that of the medication-taking group. Therefore, these data were collected from patients with an observation period of 1 year or more.
Audiologic evaluation
Based on the above criteria of interval of data collection, the patients’ initial PTA and PTA for each interval were collected.
The PTA information was collected at frequencies of 250, 500, 1,000, 2,000, 4,000, 8,000 Hz, and based on PTA, a quaternary method was derived.
Additionally, the date of each visit was checked, and the date interval was calculated. The study start date, study end date, first observation date, last observation date, event, andsurvival time were collected for use in the Kaplan–Meier curve. That information is as follows:
1) Study start date: January 1, 2015, the date of commencement of medical profile collection;
2) Study end date: May 31, 2021, the date of end of medical profile collection;
3) First observation date: It was designated based on the date of diagnosis;
4) Last observation date: It was designated based on the last visit during the investigation period (January 1, 2015, to May 31, 2021);
5) Event: Event simply states that the patient is not getting better. This concept can be divided into two options. First, it is an event if it came within the wash-out period or if a reservation was made at a later date regardless of the study period (investigation period+wash-out period). This is because, if there is a history of visitation during the wash-out period or a scheduled visitation is set, it can be considered that the treatment has not been completed. The second is a case in which the hearing did not improve. That is judged based on the severity criteria of PTA (mild, moderate, severe, and profound) [24]. Based on these grading systems, if the grade deteriorated or remained the same, it was marked as an event; and
6) Survival time: The survival time was calculated based on the concept of the event, and the difference from the first observation date was calculated by measuring the date of the event. In the case of absence of an event, the difference between the last observation date and the first observation date was calculated.
Statistical analysis
The following information of the patients was used: medical history including hypertension, diabetes mellitus, tinnitus, dizziness, initial and final PTA, sex, age, duration of treatment, ear side, medications (either monotherapy or combination therapy), and the date of initial diagnosis. All variables were processed by SPSS statistics for Windows (Version 25.0 IBM Corp., Armonk, NY, USA). The continuous variables were analyzed using parametric statistical method, such as the independent t-test. Additionally, the categorical variables were analyzed using nonparametric statistical methods, such as the chi-square test. To compare the survival time of Ginkgo biloba monotherapy and Ginkgo biloba and choline alfoscerate combination therapy, the Kaplan–Meier curve technique was used. A p-value <0.05 was defined as statistically significant.
Results
Numbers of the enrolled patients
The enrolled patients were divided into four groups at intervals of 3 months: 1) Group A including the patients extracted in the study period between 3 to 6 months; 2) Group B including patients extracted in the study period between 6–9 months; 3) Group C including patients extracted in the study period between day 9–12 months; and 4) Group D including patients extracted in the study period between day 12–15 months (Table 2).
The negative control group included 60 patients. The negative control group could not divide into the four group, as above because PTA could not be measured every 3 months in this group because their follow-up interval was longer as mentioned above.
General characteristics of enrolled patients
Table 3 shows the general characteristics of the enrolled patients. In the row information of Table 3, age was written as mean age±standard deviations, sex was the number of men and women in the group included in the experiment, and the ear side indicates how many right and left sides of the ear were included in the experimental group, respectively. Additionally, regarding the underlying diseases, hypertension, diabetes mellitus, tinnitus, and dizziness were listed, which included the number and proportion of patients in each group. The p-value is the result of comparing each item between each group.
Results of variables related to pure tone average and treatment duration
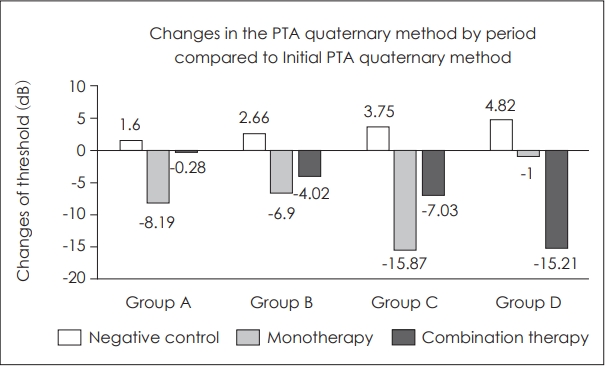
Fig. 1 shows the changes in the PTA quaternions for each section compared to the initial PTA. It was calculated as follows: final PTA – initial PTA.
In the case of the negative control group, as mentioned above, there were no follow-up data for each section; therefore, the degree of deterioration was calculated proportionally under the assumption that audition deteriorates in a linear function.
Therefore, since Group A corresponds to a period of 3 to 6 months, its period was represented by a median value of 135 days. According to the same principle, periods of Group B, Group C, and Group D were estimated by the median values of 225 days, 317.5 days, and 410 days, respectively.
Table 4 shows the results of variables related to the pure tone average and treatment duration.
Significant results are observed in Group A among of duration of treatment, and all options of variables of the PTA gradient gap. Within each group (Group A, B, C, D), the gradient is calculated as follows:
Gradient = (final PTA–initial PTA)/duration of treatment.
As can be seen in the formula, the greater the gradient, the greater the degree of hearing deterioration. Through the gradient of each group, the differences between groups were calculated; in other words, the gradient gap was calculated. Gradient gap means that the greater the difference, the faster the hearing deteriorates as time goes by.
As shown in Table 4, the gradient gap of monotherapy group between neighboring groups was 4.14±0.13, 2.81± 0.07, 2.16±0.01, respectively; and the gradient gap of combination therapy between Group A, B, C, and D is 0.03±0.10 (Group A–B), 1.18±0.08 (Group B–C), and 1.20±0.08 (Group C–D), respectively. Additionally, p-value of all three groups was <0.001, which means significant statistical results.
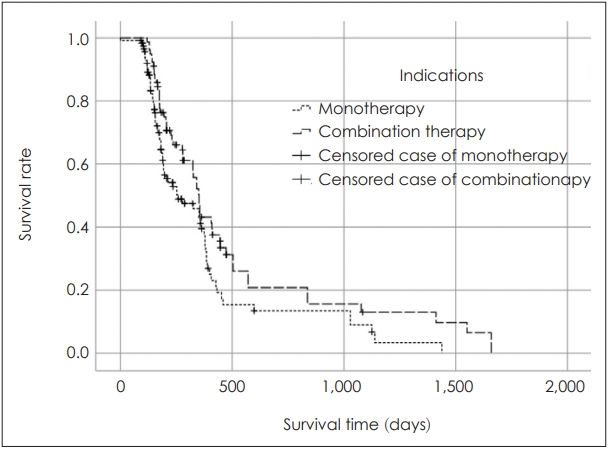
Result of comparison of Kaplan-Meier survival curves between groups
Fig. 2 shows the results of the Kaplan–Meier curve. In case of presbycusis, the meaning of survival time can be thought as deafness. It also contain basic information of the Kaplan–Meier curve with significance in Fig. 2. When comparing the survival time between these two groups, combination therapy had a significantly longer survival time.
DISCUSSION
The prevalence of hearing loss is on the rise, and in some ways, it is an inevitable disease as part of aging. Currently, various treatments have been proposed and are being studied; however, there is no clear way to restore hearing [8]. In such a situation, slowing the rate of hearing loss can have clinical significance because it means preventing hearing loss as much as possible. In other words, there are treatments that have been tried recently, as mentioned above; however, prevention is still a priority at present. In a such scenario, through this study, Ginko blioba monotherapy compared to the negative control group that did not use any drug, and combination therapy resulted in a slower rate of hearing loss.
Looking a little more closely at the PTA gap and gradient of the results, first, the PTA gap is the PTA measured at the time of patient visits. Additionally, the PTA at the time of the first visit and at the time of the last follow-up is identified. It means that the PTA of the last follow-up period subtracted from the initial PTA. That is, it is possible to quantify the change of the patient’s hearing level. However, this is merely a difference and does not reflect how quickly it deteriorated. So, by measuring the speed and its difference, knowing how much change over how much time is important for more detailed comparison. For example, suppose two cars traveled 100 m in 10 s and 100 s respectively; although the distance traveled is the same, the speed is 10 times different because the time is 10 times longer. As such, the PTA is not a simple change; however, how much the PTA changed over time is important to know. So, the gradient was introduced as a concept, and the gradient is the difference between the patient’s PTA difference by initial and last follow-up intervals divided. Thus, when this concept was introduced, it was confirmed that the combination therapy had a more significant meaning than the monotherapy group and the monotherapy group than the negative control group in terms of the speed of the gradient that worsens hearing. It can also be confirmed by the results of the Kaplan–Meier survival curve. Additionally, this brings us to the query of what it means for this rate of deterioration to decrease. If hearing is understood numerically, it is hearing that gets better, stays present, or gets worse. However, as a natural phenomenon of aging, hearing deteriorates rather than maintaining at the same level over time, and there is currently no way to improve hearing. Therefore, if the rate of hearing deterioration can be slowed, the rate of aging in terms of hearing can be slowed. It can be interpreted as not only the rate of decreasing hearing deterioration, but also slowing the onset and progression of various diseases related to the deterioration of hearing. One example of slowing the rate of deterioration is mild cognitive impairment. The drug donepezil can slow the deterioration of mild cognitive impairment, which greatly improves the quality of life by slowing the morbidity to severe dementia [25]. As such, simply slowing the rate of deterioration of hearing does not end with hearing problems but may slow the onset and progression of other related diseases. It can be seen that it has a potential effect.
Meanwhile, as shown in previous studies, there have been no significant results in PTA related studies with Ginkgo biloba monotherapy [26]. Therefore, a combination therapy using additional drugs is needed rather than Ginkgo biloba alone. In this study, by adding choline alfoscerate, a model combination therapy was established and statistically verified, wherein significant results were derived. The next query is regarding mechanism by which this combination therapy could affect the rate of hearing deterioration. This can be estimated by looking at the mechanism of each drug. Ginkgo biloba acts in diverse mechanisms, a vaso-regulatory effect promoting increased blood flow, antagonism of the platelet activating factor, which plays a role in oxygen radical production, has antioxidant activity, including scavenging of free radicals, enhancing neuronal plasticity, and anti-inflammatory effects and protective actions against brain damage. With respect to neuropathy, according to an animal model study with Ginkgo biloba, it reduces or inhibits monoamine- oxidase activity, which metabolizes dopamine, induces the formation of free radicals, and leads to damage of nigrostriatal neurons. Another mechanism related to neuropathy is the neuroprotective effect of EGb761 against 6-hydroxydopamine, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine, and MPP+ toxins [27]. Additionally, choline alfoscerate increases the synthesis and release of cerebral acetylcholine [28]. It is thought that each of these mechanisms exerts a complex effect and puts the brakes on the rate of hearing deterioration.
There was no case of discontinuation of the drug due to the side effects among the patient groups included in this study. The commonly found side effects of Ginkgo biloba include headache, dizziness, heart palpitation, upset stomach, constipation, and allergic skin reactions. Additionally, caution has to be exerted when alprazolam, anticonvulsants, and antidepressants are taken together with Gingko biloba [29]. The side effects of choline alfoscerate include heartburn, headache, dizziness, and skin rash [30]. The fatal side effects currently reported are not common; therefore, long-term use is thought to be feasible, However, the follow-up period of this study is up to 1 year and 6 months; therefore, if future research is conducted in the form of longer-term observations, the effect on long-term use will also become known. Although we can conclude that it delays the rate of hearing deterioration, it is still unclear as to, whether it is simply related to hearing, or if it is due to an improvement in the cognitive ability due to complex cognitive improvement. It is yet to be determined whether it is a relative synergistic effect of hearing. Therefore, by using additional methods such as speech audiometry, future studies can the relationship with not only hearing but with cognitive ability.
Limitation
As mentioned above, if more samples were collected in Fig. 1, the trend could have been better represented. Most of the samples are concentrated in Group A, and the number of sample groups tends to decrease sharply as we move on to Group D. Therefore, to increase the number of samples as a whole and to create a uniform sample between groups may be a limitation.
Also, in Fig. 1, although except for Group D, the trend was approximately consistent; however, if more samples were collected, it probably would have brought out statistically different results. The presence of hearing aids would affect the prognosis of patients with medications, but we could not collect the data in patients in this retrospective study.
In addition, this study was not conducted with patients over a period of 15 months; notably, if patients over a period ≥15 months are properly collected and included in the study, it may derive more long-term results between monotherapy and combination therapy.
Conclusion
At this point in time when there is currently no clear treatment, Ginkgo biloba and choline alfoscerate combination therapy may be a treatment option. In the future, it is expected that the mechanism and effect will be elucidated in more detail, so that it can become an option for treatment.