Introduction
Cochlear implantation (CI) effectively restores hearing, facilitates language development and improves the quality of life [1]. Accumulating evidence shows that language development is optimal when CI is performed early [2]. Preoperative residual hearing in prelingually deaf children enhances speech perception after CI [3]. Although the identification and preservation of residual hearing are important, behavioral audiometry is not appropriate for some CI candidate children [2,4]. For children who cannot undergo such audiometry, the click or tone burst auditory brainstem response (ABR) is widely used as an objective hearing measurement method. ABR stimuli are transient, not frequency-specific, and its maximum output is 90 dB [5]. Thus, the ABR test has certain limitations when used to assess residual hearing in those who are severely to profoundly deaf [5]. The auditory steady state response (ASSR) is a scalp-recorded auditory evoked potential elicited in response to sinusoidal and/or frequency-modulated tones [6]. The ASSR test complements the limitations of the ABR test: stimuli are narrowly defined in terms of frequency, the maximum stimulation is 120 dB because the stimulus is of long duration, and the results are delivered automatically [5,7-9]. Thus, the ASSR test is useful for estimating the hearing thresholds of patients exhibiting no ABR at the maximum stimulus [10].
Patients lacking ABRs are generally considered deaf. However, some exhibit ASSRs. Residual hearing on ASSR enhances the outcomes of CI in children with inner-ear malformations [7]. To the best of our knowledge, no study has yet analyzed the effects of residual preoperative ASSR hearing on CI outcomes in children with severe to profound hearing loss; this is the topic of this study.
Subjects and Methods
We retrospectively reviewed the relationship between the preoperative ASSR and the post-CI outcomes of children lacking ABRs. The study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 1811-102-987).
Study material
Of all patients less than 60 months old who underwent CI (Nucleus CI 422 device) at Seoul National University Hospital (Seoul, Korea) from January 2015 to July 2017, those who lacked ABRs in both ears were initially enrolled. The inclusion criteria were the availability of preoperative ASSR and post-CI mapping data at 3 months and 1 year postoperatively. The exclusion criteria were the presence of any inner-ear anomaly, any surgical complication, developmental delay, or a comorbidity that might affect post-CI outcomes. For each frequency at 0.5, 1, 2, and 4 kHz, all ears were divided into two groups by reference to the preoperative ASSR data: a residual hearing group (ASSR thresholds ≤110 dB at all frequencies) and a hearing loss group (no ASSR response upto 110 dB stimulation). At each frequency, the perceptional threshold (T-level), comfort level (C-level), and electrical dynamic range (EDR) were measured 3 months and 1 year postoperatively, and compared between the two groups.
We also compared hearing and speech evaluation data. Of all patients, those who underwent simultaneous bilateral CI were divided into two groups: group 1 (all response group) contained patients who exhibited ASSR thresholds at all frequencies in both ears; group 2 (partial response group) lacked ASSR at least one frequency in any ear. The maximum ASSR stimulus was 110 dB, and when there is no ASSR at 110 dB, it is assumed to be 120 dB and the mean ASSR threshold was calculated. Categories of Auditory Perception (CAP) scores and Infant-Toddler Meaningful Auditory Integration Scale (IT-MAIS) scores in terms of speech perception were recorded preoperatively, and 3 months and 1 year postoperatively, and compared between the groups. Patients who did not undergo postoperative 3-month or 1-year hearing and speech evaluations at our center were excluded.
ABR
ABRs and ASSRs were tested using a Bio-logic MASTER II platform (Navigator Pro, Bio-Logic, San Carlos, CA, USA). All children lay on a bed in a soundproof room and were sedated with oral pocral syrup (50 mg/kg). Electroencephalographic activity was recorded using gold disk electrodes placed on the mastoid and high forehead or vertex. The ground was placed on the forehead. The inter-electrode impedance was <3-5 kΩ. Click stimuli (duration: 100 ms) were presented through ER3A inset earphones (Etymotic Research Inc., Elk Grove Village, IL, USA) at a maximum of 90 dB HL at 11.1-32.1/s with alternating polarity. Thresholds were determined at 5 dB intervals. A response was considered absent when the 90 dB wave triggered no response.
ASSR
Surface recording electrodes were placed on the forehead (ground) and the mastoid (reference). A disk electrode was placed at the vertex (active). The electrode impedances were <5 kΩ. Air-conducted stimuli were presented to both ears via ER3A inset earphones. Four carrier frequencies were tested (0.5, 1, 2, and 4 kHz); all were 100% amplitude-modulated and 20% frequency-modulated at modulation frequencies of 82, 87, 91, and 96 Hz (left side) and 84, 89, 94, and 99 Hz (right side), at intensities ≤80 dB HL. At intensities ≥90 dB HL, the modulation frequencies were 67 Hz (left side) and 69 Hz (right side). The maximum presentation level was 110 dB HL. During each recording, 16-32 sweeps were made in each block; data were averaged in the time domain and subjected to fast Fourier transformation. Response level significance was set to p<0.05 and was monitored after each sweep.
Mapping
The mapping strategy was identical for all patients (advanced combination encoder, monopolar 1+2; pulse width=25, sensitivity=12). For each patient, the T-level was the lowest current level (CL) eliciting an auditory sensation. The C-level was the highest CL that was not uncomfortably loud. The EDR was the difference between the C- and T-levels [11]. The electrical channels delivered data derived at various frequencies; electrodes 20, 16, 11, and 6 yielded most data for 0.5, 1, 2, and 4 kHz, respectively. A CP 920 processor or CP950 Kanso processor (Cochlear Ltd., Sydney, Australia) were used.
Auditory performance evaluation
Hearing was evaluated at 3 months and 1 year postoperatively, depending on patient age. The CAP score lies on an eight-point hierarchical scale ranging from no awareness of environmental sound (category 0) to conversational use of the telephone with a known speaker (category 7) [12]. The IT-MAIS score was calculated based on the answers given by caregivers; the instrument includes 10 items in three domains: vocalization behavior (items 1-2), alerting to sounds (items 3-6), and deriving meanings from sounds (items 7-10). Each item is scored from 0 to 4: 0, never; 1, rarely (25%); 2, occasionally (50%); 3, frequently (75%); and 4, always (100%) [13].
Statistical analyses
The independent-samples t-test was used to compare the Tand C-levels and the EDRs of the two groups at 0.5, 1, 2, and 4 kHz. The correlations between T- and C-levels, and ASSR thresholds, were analyzed via simple linear regression and calculation of Pearson correlation coefficients. The Mann-Whitney U-test was employed to compare the CAP and IT-MAIS scores. A p-value<0.05 was considered to reflect statistical significance. All analyses were performed using SPSS software (ver. 20.0; IBM Corp., Armonk, NY, USA).
Results
Post-implant mapping results
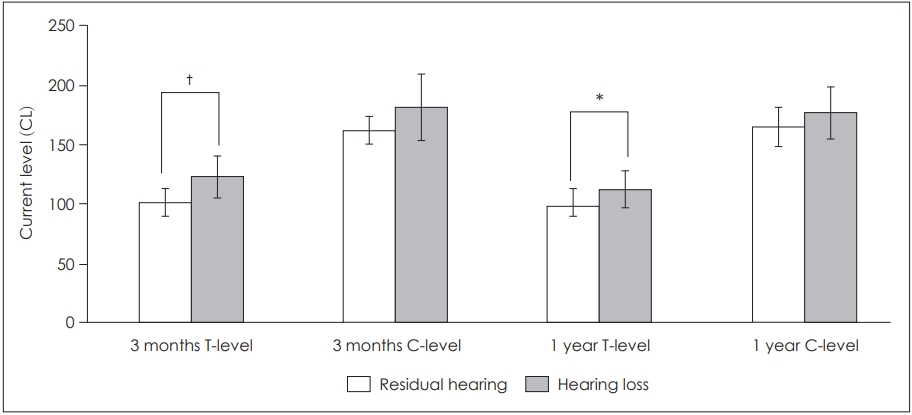
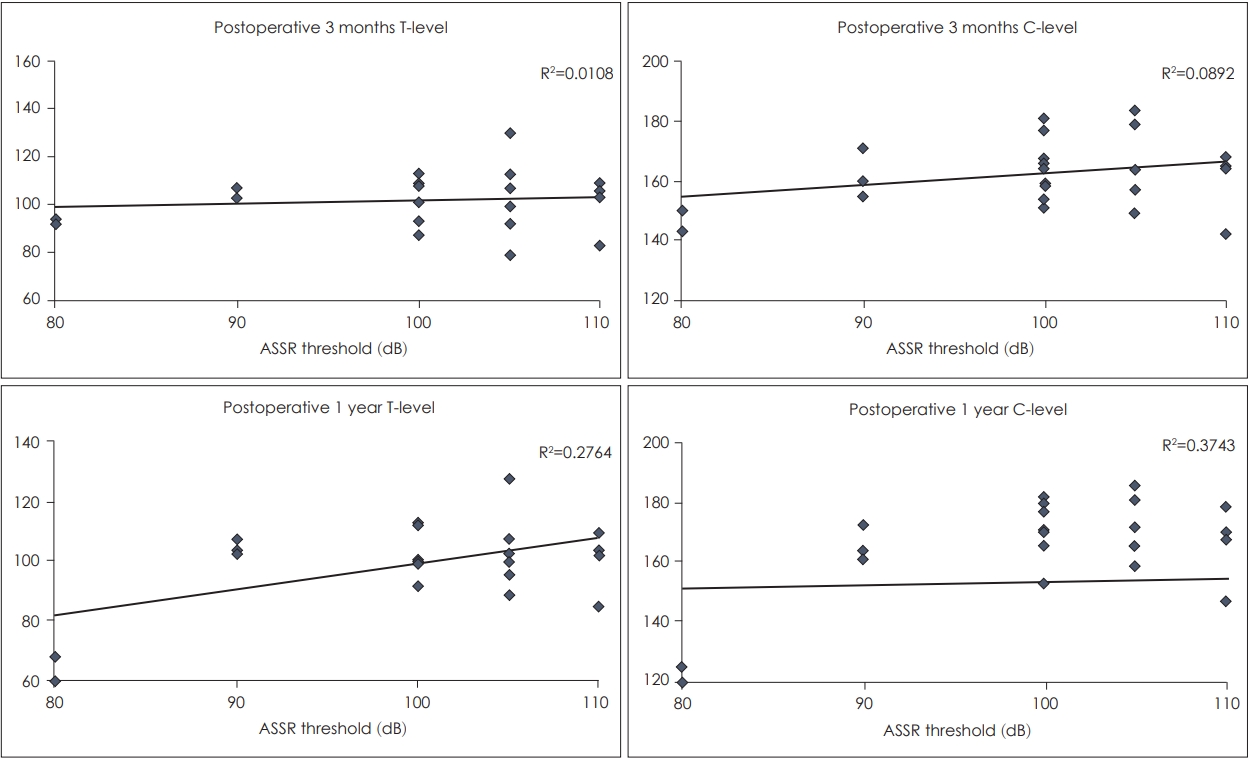
We enrolled 16 patients (4 boys and 12 girls; 30 ears, 8 boys’ and 22 girls’) with a mean age of 17.0±5.7 months. Thirteen underwent simultaneous CI, one underwent CI of both ears in 1-year interval, and two underwent right-ear CI only. At each frequency, all ears were divided into those with and without residual hearing. At all frequencies, the mean age and sex distributions of the two groups did not differ significantly (Table 1). At 2 kHz, a significant relationship was apparent between the preoperative ASSR and the post-CI outcome. At 2 kHz, the postoperative 3-month and 1-year T-levels of those with residual hearing were lower than those of patients with no hearing (p=0.001, p=0.035) (Fig. 1). Simple linear regression showed that the ASSR threshold correlated positively (but weakly) with the postoperative 1-year T-level (p=0.012, R2=0.276) and C-level (p=0.002, R2=0.374); the C-level correlation was better (Fig. 2).
Auditory performance
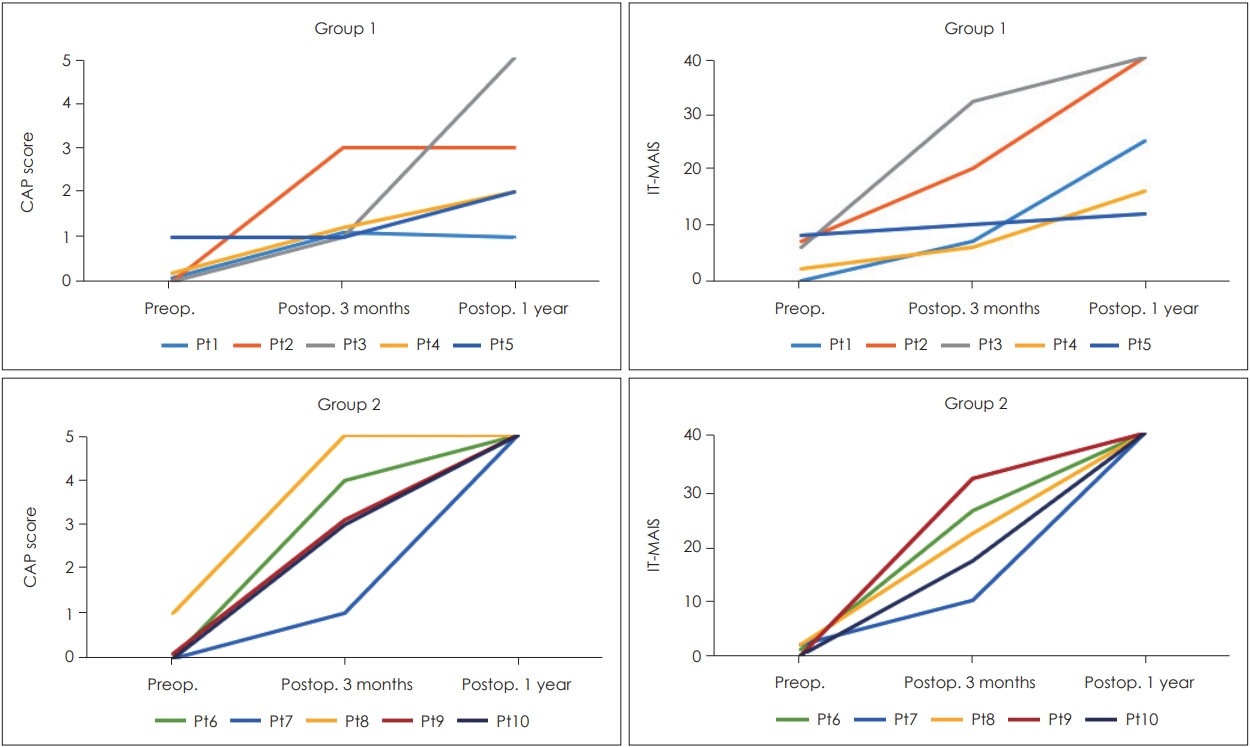
Of the 13 patients who underwent simultaneous bilateral CIs, 3 were excluded because of the absence of speech evaluation data. The remaining 10 patients were divided into group 1 (responses at all frequencies, n=5) and group 2 (no response at ≥1 frequency, n=5). The mean patient age at the time of CI was 14.9 months, but group 1 patients tended to undergo CI later (17.6 months vs.12.2 months, p=0.105) (Table 2). Compared to group 1, group 2 exhibited a significantly higher CAP score at the postoperative 1-year speech evaluation (2.6 vs. 5.0, p=0.018); the IT-MAIS score was also higher in group 2, but statistical significance was not attained (26.6 vs. 40.0, p=0.054). All group 2 patients achieved CAP scores of 5 and IT-MAIS scores of 40, but patients 1, 2, 4, and 5 of group 1 did not attain such scores (Fig. 3).
Discussion
We investigated the effects of ASSR residual hearing on the CI outcomes of children lacking ABRs. When the ABRs are bilateral absent, the possibility of residual hearing is not precluded [14]. We found that ASSR residual hearing improved CI outcomes. ASSRs yield useful information on children lacking ABRs. However, the group with residual hearing on ASSR exhibited a significantly poorer CAP score 1 year postoperatively.
First described by Galambos et al. in 1981, ASSR testing has evolved considerably and is now widely used [15,16]. Strong correlations are evident between behavioral audiometry and ASSR data; the differences fall as the severity of hearing loss increases [17-23]. The mean differences between the ASSR and behavioral thresholds are 0-17 dB for adults with normal hearing and 5-13 dB for those with mild to severe sensorineural hearing loss (SNHL) [15]. Rance and Briggs [22] reported significant positive correlations (r=0.81-0.93) between ASSR and behavioral hearing thresholds at 250-4,000 Hz in 184 infants with moderate to profound SNHL. Han, et al. [23] also reported strong correlations (r=0.91-0.93) between these two measurements in 40 young children (aged 6 months to 5 years) with SNHL. Beck, et al. [21] reported that, among pediatric CI candidates, the mean difference between the ASSR and behavioral thresholds was 0.09-8.94 dB, and an absent ASSR was a strong predictor of profound hearing loss as evidenced by the behavioral threshold (specificity >90%).
Preoperative residual hearing evident in behavioral audiometry improves speech perception and language development after CI in prelingually deaf children [3]. Several studies have explored the effects of residual preoperative hearing on the outcomes of electrophysiolocal procedures and CI. Kileny, et al. [24] found that the preoperative, electrical, promontory stimulation threshold predicted post-CI speech and sound recognition in 10 patients. Jeon, et al. [25] reported that patients with auditory neuropathy spectrum disorder who exhibited electrically evoked auditory brainstem responses (EABRs) performed better after CI (in terms of the CAP score) than those lacking EABRs. Kuo and Gibson [26] reported that CI recipients aged 10-15 years old found it more difficult than younger children to learn speech perception and production. However, in such patients, residual hearing at 2-4 kHz prior to CI correlated positively with more rapid improvement [26]. Cowan, et al. [27] reviewed 117 children who had undergone CI and found that those with better preoperative residual hearing scored significantly higher on open-set word and sentence perception tests when using the implant alone. Qiao, et al. [7] studied 72 children with inner-ear malformations who received multichannel CIs. At low, moderate, and high frequencies (0.5, 1-2, and 4 kHz, respectively), the behavioral T-levels 1 year after implantation were significantly lower in those with residual hearing compared to those with hearing loss (p<0.01) [7]. They found that the preoperative ASSR thresholds significantly correlated with the postoperative EABR thresholds (p<0.01, r=0.48-0.88).
The 2 kHz T-level after CI differed significantly between those with and without residual hearing. We also found weak associations between the ASSR threshold and the postoperative 1-year T- and C-levels. At other frequencies, we found no such relationship. One possible explanation is that the 2 kHz ASSR test measures residual hearing more accurately than ASSR tests at other frequencies. Although ASSR and behavioral audiometry data are well-correlated, the ASSR test may underestimate residual hearing to greater extent than behavioral tests [28]. Compared to behavioral audiometry, the ASSR at 2 kHz was associated with higher positive and negative predictive values than at other frequencies [18]. In CI candidates aged 6-72 months old, the 2 kHz ASSR test exhibited a higher sensitivity and specificity and a lower mean difference than did visual reinforcement audiometry [21]. However, artifact-like responses to high-intensity ASSR tests, particularly at 0.5 and 1 kHz, may introduce errors [10,29]. In addition, the hearing loss group may have included patients with hearing thresholds >110 dB. To avoid cochlear damage, we set the maximum stimulus to 110 dB [21]. Neither the T- nor C-level stabilizes for several months after CI; children require more time than adults [30]. The C-level reflects a loud but comfortable level. The T-level reportedly stabilizes earlier and is more reliable than the C-level [30].
We found that residual hearing on ASSR was significantly (negatively) related to the 1-year postoperative outcome. In addition, the CAP and IT-MAIS scores tended to be higher in patients who lacked an ASSR at ≥1 frequency, although statistical significance was not attained (this was the opposite of what we expected). However, as shown in Fig. 3, patients 4 and 5 (who underwent CI 21 and 24 months old respectively, older than other patients) greatly affected the results. It is well known that early implantation to stimulate the hearing pathway during sensitive period for language acquisition gives deaf children the best chance to close the language gap to their peers [2]. Speech perception and language development after CI are also affected by multiple factors including the educational environment and the extent of family engagement in therapy [3]. Thus, we believe that age at implantation, consistency of CI usage, and efficacy of post-CI therapy all markedly affect speech perception. CI should not be delayed even though marginal residual hearing is evident in the ASSR test.
Our study had certain limitations. Our sample size was small. Because our patients were young at the time of CI, most could not undergo behavioral audiometry or speech evaluation using the Phonetically Balanced Word List, vowel or consonant tests, or a sentence test.
In conclusion, for child patients who exhibited hearing loss in preoperative ABR evaluations, residual hearing on ASSR at 2 kHz improved the post-CI T-level. Weak associations were apparent between the ASSR threshold and the postoperative 1 year T- and C-levels. Of patients who underwent simultaneous bilateral CIs, those exhibiting better ASSRs at all frequencies exhibited lower CAP scores at the postoperative 1-year speech evaluation, possibly because they were older at the time of operation. Thus, we strongly recommend CI even though there is marginal residual hearing from ASSR test in child patients.