Introduction
Carcinomas of external auditory canal (EAC) are very rare with an annual incidence of around 1 per million people.1) Even large centers only see few patients. Because of the rarity, consensus regarding the treatment of carcinomas of EAC is inadequate. Although some progress in treating this disease has been made over the decades, guidelines and treatment protocols are still needed. Among these tumors, basal cell carcinomas are less frequently noted than squamous cell carcinomas.
The authors will describe a case of basal cell carcinoma located in the EAC and the treatment experience with a review of the literature.
Case Report
A 55-year-old female in otherwise good health presented with a 10-year history of an intermittent otorrhea in the right ear.
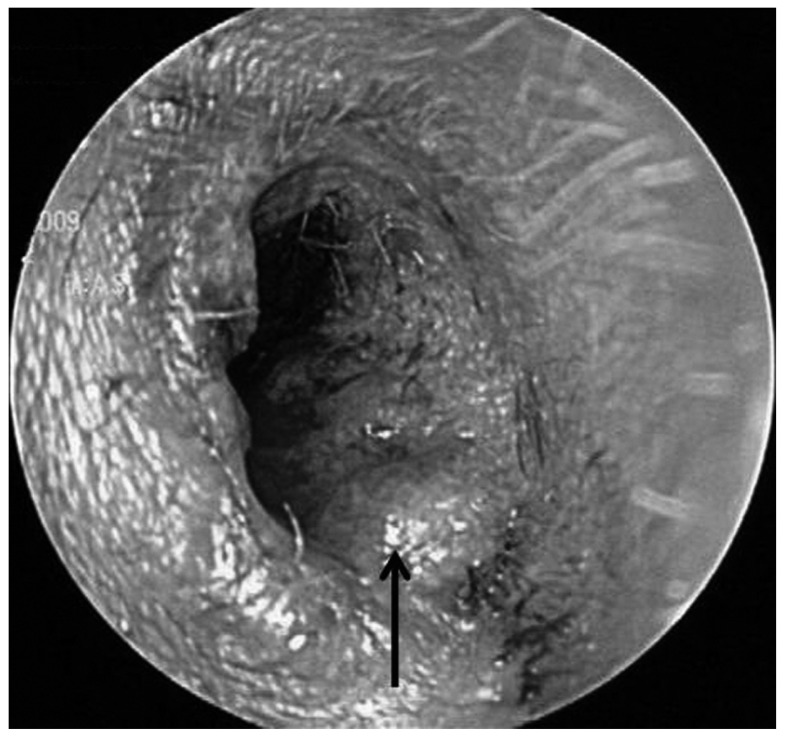
A physical examination revealed a small nodular mass arising from the posterior inferior aspect of the right cartilaginous portion of the EAC (Fig. 1). Right tympanic membrane was intact.
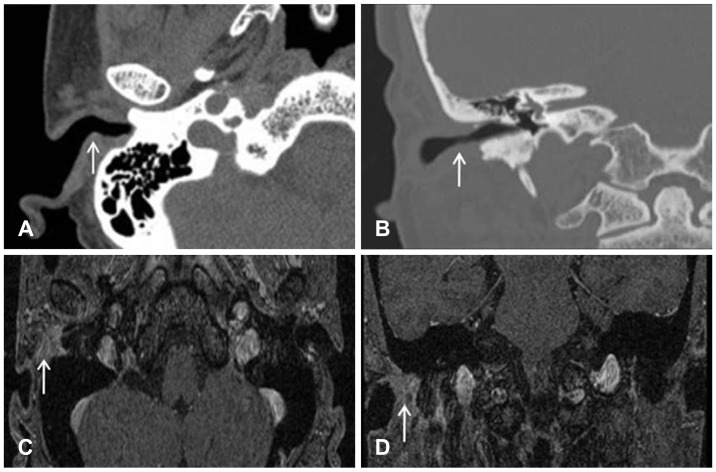
Other clinical examinations including the head and neck region, laboratory findings, and audiologic findings were within normal limits. It appeared to be a benign lesion of EAC, an excisional biopsy was performed under local anesthesia. Contrary to expectation, histologic examination was interpreted as a basal cell carcinoma (Fig. 2). Fortunately, surgical margin was negative for malignancy. Further evaluation of the temporal bone by computed tomography (CT) and a magnetic resonance imaging (Fig. 3) of the head and neck showed no involvement of any other temporal bone or of head and neck structures.
Although less probable, because distant metastasis cannot be ruled out completely, a full metastatic workup was done. Bone scan, hepatobilliary sonography, duodenoscopy, chest X-ray, and CT of the chest, PET-CT were all negative for signs of nodal involvement or metastases to other organs.
According to the Pittsburgh staging system,2) the patient had tumor limited to the EAC without bony erosion or evidence of soft tissue involvement (T1), no lymph node metastases (N0), and no distant metastases (M0).
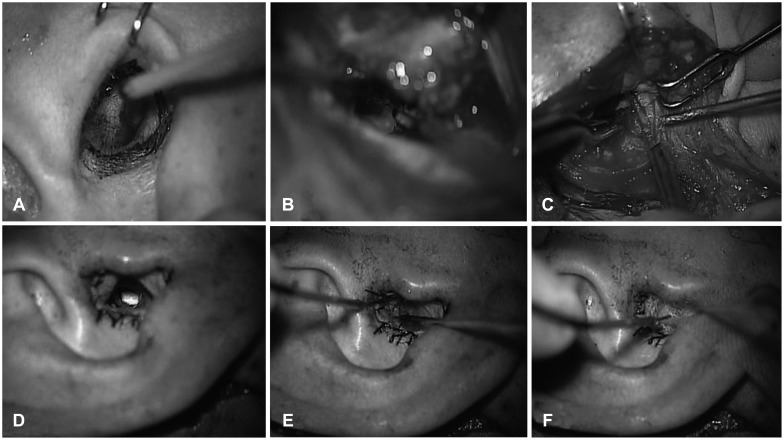
The patient underwent sleeve resection of the EAC reconstructed with a coverage of the EAC using a left thigh split-thickness skin graft (Fig. 4). Pathologic findings confirmed a basal cell carcinoma in situ not invading cartilage, all surgical margins being free of invasion (Fig. 2). No adjuvant chemotherapy or radiation was administered.
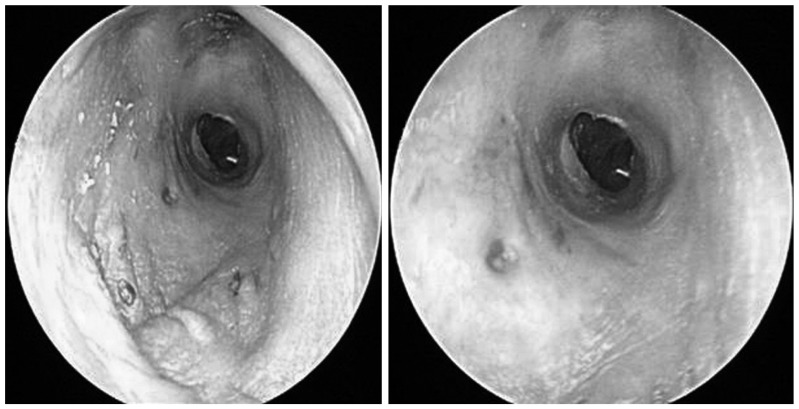
After 1 year of surgery, the patient is in good health with no evidence of complication or recurrence (Fig. 5).
Discussion
Among carcinomas of EAC, squamous cell carcinoma (SCC) is the most common, accounting for 80% of tumors within the temporal bone.3) Basal cell carcinoma, adenoid cystic carcinoma, adenocarcinoma, melanoma, and various sarcoma are among the other malignancies within the temporal bone.4)
In 1990, the Pittsburgh group proposed a staging system for SCCs of the EAC. Arriaga, et al.2) proposed a primary tumor, regional nodes, metastasis (TNM) staging of EAC carcinoma on the basis of clinical examination, and preoperative CT scan finding.2,5) Other authors have supported the clinical usefulness of this staging.6,7) The classification method proposed by Arriaga, et al.2) is advantageous with regard to treatment, because it correlates the clinical and radiologic characteristics in patients.
Because of the rarity of malignant tumor of EAC, there are no randomized clinical trials. Therefore, the management of these tumors is difficult. In the several studies, authors disagree about the extent of surgery and the role of radiotherapy and chemotherapy in managing these tumors. Gidley8) reviewed several literatures and discussed about treatment strategies focused on the carcinoma of EAC. Early stage tumors can be managed with a surgery alone reserving radiation as a component of salvage options. Small T1 tumors that are confined to the soft tissues, cartilaginous ear canal can be removed with wide local excision, where the skin of the ear canal and the underlying cartilage are removed with frozen section medial margins. This operation must be selected for limited tumors that do not cross medially over the bony-cartilaginous junction. T1 tumors of the bony ear canal and T2 tumors (i.e., those with limited bony or soft tissue involvement) are best controlled with lateral temporal bone resection.
Basal cell carcinoma of the EAC is known to have a locally aggressive nature and lack of regional lymph node metastasis. Basal cell carcinomas are less lethal because of their slower growth rate and rare metastasis.9,10) Because there is a possibility of distant metastasis, evaluation must be completed before treatment plan is established. In 2002, Nyrop and Grøntved11) evaluate the result of surgically treated cancer of EAC in twenty consecutive patients. The authors concluded that the outcome was related to the stage of disease, suggesting that the Pittsburgh staging system is also useful in patients with non-SCC.
Patients with early cancer benefited from less aggressive surgical approach, while survival was poor in patients with an advanced cancer who went through a more aggressive surgery despite adjuvant radiotherapy.9,12)
Fortunately, our patient had tumor limited to the EAC without bony erosion or evidence of soft tissue involvement (T1), no lymph node metastases (N0), and no distant metastases (M0).
Using the treatment strategies described above on the carcinoma of the EAC, we can remove the tumor with a minimal safety margin and have better treatment results.